
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
Castleman Disease
Introduction:
- It is a rare group of lymphoproliferative disorders with characteristic histopathological appearances.
- Also called as “angiofollicular hyperplasia”.
Etiology:
- HHV-8 infection- Commonly seen in immunodeficiency status such as HIV
- Association with POEM's syndrome- Malignant plasma cells induce Castleman's disease type lymphadenopathy. They generally have IgG or IgA paraprotein with lambda chain restriction. Thrombocytosis and elevated VEGF levels are consistently present. These cases need autologous stem cell transplantation.
- Idiopathic CD- Those cases which are not associated with HHV-8 or POEM's syndrome. TAFRO (Thrombocytopenia, Anasarca, myeloFibrosis, Renal dysfunction and Organomegaly) is a perticularly aggressive form of idiopathic CD.
- Other diseases with Castleman Disease like histology include:
- Infections: EBV, Mycobacteria, Toxoplasmosis, CMV
- Autoimmune and inflammatory: IgG4 related disease, SLE, RA, Adult onset Still's disease
- Neoplasia- Kaposi sarcoma, Mantle/ Marginal zone lymphoma, Germinotrophic lymphoproliferative disorder.
Pathogenesis:
- Immunodeficiency status facilitates replication of HHV-8 in blastic cluster of CD20 positive lymphocytes
- Viral genome expresses several genes which
- Inhibit apoptosis- LANA-1, vFLIP, vCyclin
- Enhance cell cycle entry
- Angiogenesis
- B cell proliferation
- Excessive secretion of viral IL-6 which in turn increases release of
- VEGF
- CXCL-13
- Hepcidin
Classification:
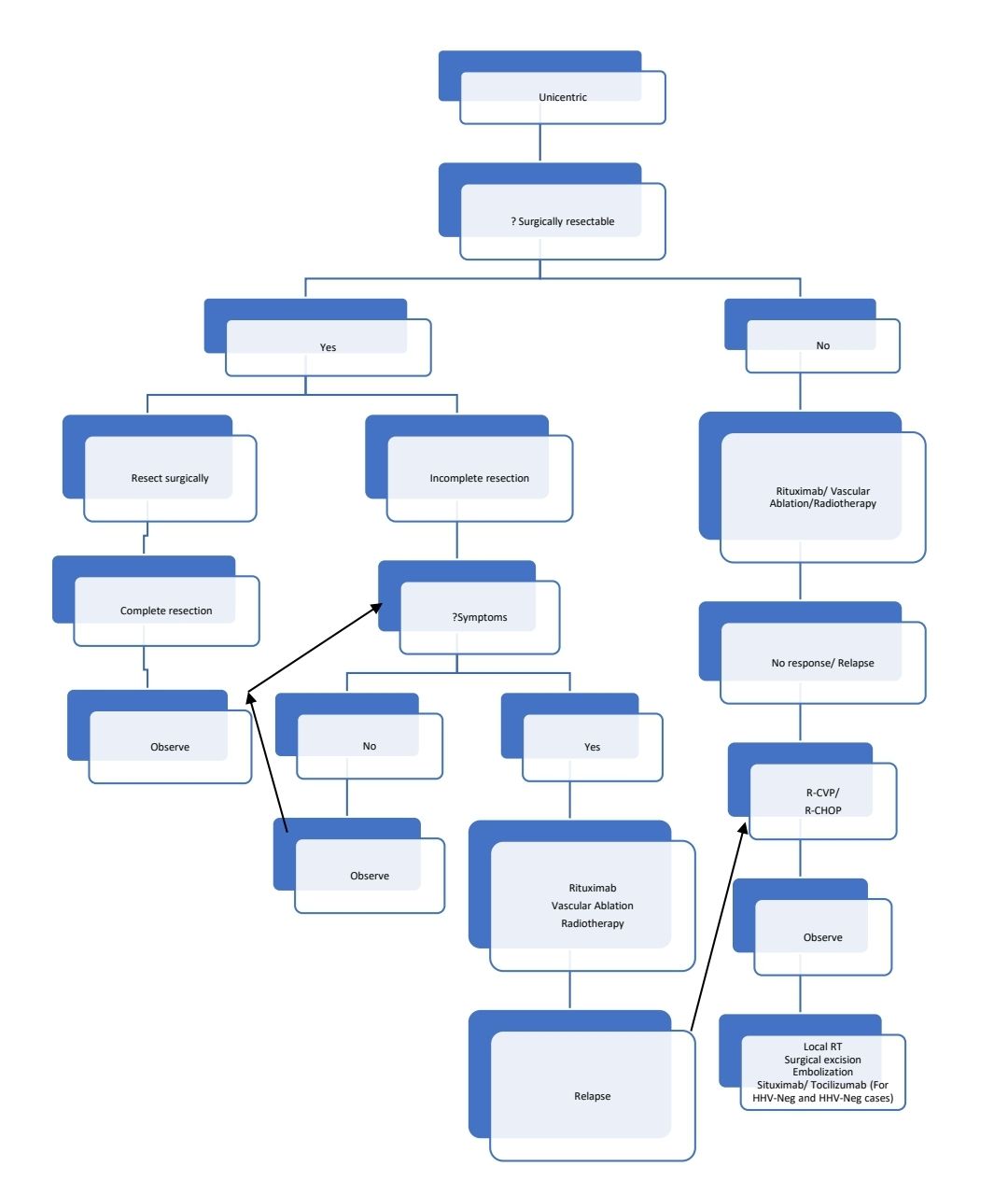
- Unicentric
- Hyaline vascular
- Plasmacytic/ Mixed
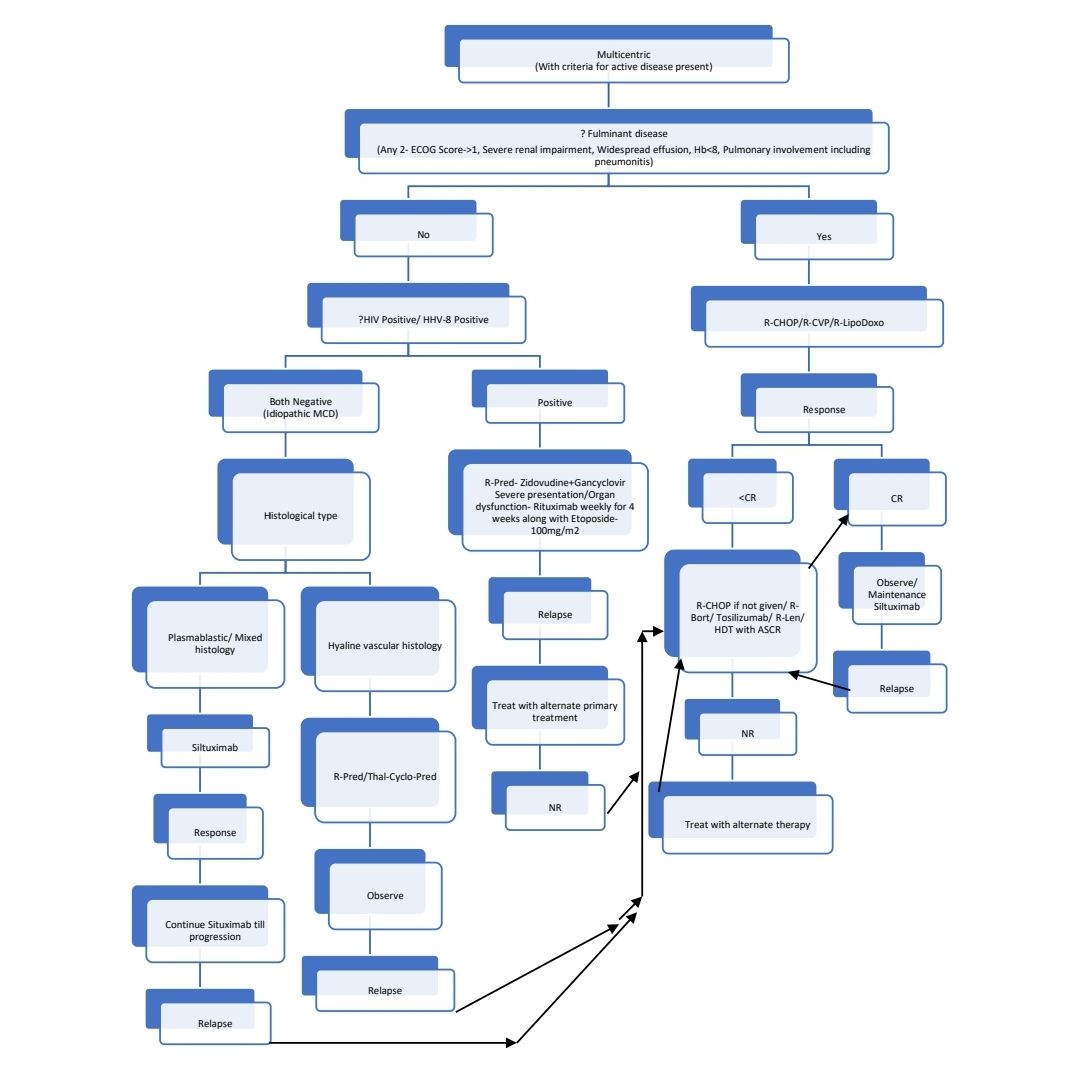
- Multicentric
- Idiopathic
- TAFRO
- NOS
- POEMS
- KSHV/ HHV8 associated
- HIV- Positive
- HIV- Negative
- Idiopathic
Clinical Features:
- Diffuse lymphadenopathy- Usually invlolving nodes in chest and neck
- Fever
- Weight loss
- Fatigue
- Dyspnea, edema, pulmonary fibrosis
- Hepatosplenomegaly
- Skin lesions- Cherry red colored eruptions
- Kaposi’s sarcoma is present in up to 70% of individuals with multicentric disease at diagnosis
Investigations:
- Lymph node biopsy
- Regressed/ atrophic/ atretic germinal centres
- Expanded mantle zone with concentric rings of lymphocytes in "onion ring" pattern
- Prominence of follicular dendritic cells
- Increased vascularity with prominent endothelial cells
- Sheetlike, polytypic plasmacytosis in the interfollicular space
- Hyperplastic germinal centres
- Plasmablasts are immunopositive for OCT2 and IIRF4/MUM1 but lack PAX5, BCL6 and CD138. They express IgM with monotypic lambda chain expression. Expression of LANA-1 confirms etiology as HHV-8.
- Histological differential diagnoses include: on-specific lymphadenitis with polytypic PCs; autoimmune lymphadenitis; reactive follicular and para-cortical hyperplasia; lymphoproliferative disorders including lymphoplasmacytoid lymphoma, plasmacytoma, follicular lymphoma and angioimmunoblastic T-cell lymphoma; follicular dendritic cell sarcoma and Kaposi sarcoma
- Biopsies have to reported by experienced hematopathologists. Online resources for reporting available at: http://cdcn.org/pathology-toolkit/
- Complete hemogram: Anemia, cytopenias
- SPE- Polyclonal hypergammaglobulinemia
- LFT- Hypoalbuminemia
- ESR, CRP- Increased
- S. Ferritin- Elevated
- DCT- May be positive
- Lymph node biopsy with IHC for LANA-1 which is a virally encoded protein.
- HHV-8 testing in blood by PCR. Serology doesnot reflect viral activity. High viral load correlates positively with relapse.
- Whole body imaging(CT or PET-CT): Done for differentiating Unicentric from multicentric disease and also to know extent of lymph node involvement. Saetime, lytic/sclerotic lesions of POEM's syndrome can be idetified.
Diagnostic Criteria:
Hyaline Vascular Unicentric Castleman disease:
- Major criteria (All 3 required)
- One enlarged lymph node (>1 cm in the short axis diameter) or multiple enlarged lymph nodes in one lymph node station
- Microscopy consistent with Castleman disease spectrum and shows: Grade 2- 3 regressed follicles/hyaline vascular follicles and
- Prominent stroma
- Prominent high endothelial vessels
- Relatively few plasma cells
- KSHV/HHV8 LANA IHC- Negative
- Exclusion criteria:
- Infections: HIV, KSHV/HHV8, CMV etc
- Autoimmune disorders: SLE, rheumatoid arthritis etc
- Malignancy: NHL, HL, thymoma
Mixed/plasmacytic Unicentric Castleman disease:
- Major criteria (All 3 required)
- One enlarged lymph node (>1 cm in the short axis diameter) or multiple enlarged lymph nodes in one lymph node station
- Microscopy consistent with Castleman disease spectrum and shows: Grade 2- 3 plasmacytosis (regressed follicles/ hyaline- vascular follicles may be seen)
- KSHV/HHV8 LANA IHC- Negative
- Exclusion criteria:
- Infections: HIV, KSHV/HHV8, COVID-19, syphilis etc
- Autoimmune disorders: SLE, rheumatoid arthritis, IgG4 related disease etc
- Malignancy: NHL, HL, myeloma, POEMS syndrome etc
Idiopathic Multicentric Castleman disease- NOS:
- Major criteria (All 3 required)
- Enlarged lymph nodes in at least 2 lymph node stations
- Microscopy consistent with Castleman disease spectrum and shows: Grade 2- 3 regressed follicles/hyaline vascular follicles or Grade 2- 3 plasmacytosis.
- KSHV/HHV8 LANA IHC- Negative
- Minor criteria (Need at least 2, with at least 1 laboratory criteria)
- Laboratory criteria
- Anemia (<12.5 g/dL males; <11.5g/dL females)
- Thrombocytopenia (<1,50,000/cmm) or thrombocytosis (>4,00,000/cmm)
- CRP >1mg/dL
- Renal dysfunction or proteinuria
- Polyclonal hypergammaglobulinemia
- Clinical criteria
- Constitutional symptoms
- Large spleen and/or liver
- Fluid accumulation (edema, effusions, anasarca)
- Eruptive cherry hemangiomatosis or violaceous papules
- Lymphocytic interstitial pneumonitis
- Laboratory criteria
- Exclusion criteria:
- Infections: EBV, HIV, KSHV/HHV8, COVID-19, tuberculosis etc
- Autoimmune disorders: SLE, rheumatoid arthritis, IgG4 related disease, Sjogren’s syndrome, HLH etc
- Malignancy: NHL, HL, myeloma, POEMS syndrome etc
Idiopathic Multicentric Castleman disease- TAFRO:
- Major criteria (All 3 required)
- Enlarged lymph nodes in at least 2 lymph node stations
- Microscopy consistent with Castleman disease spectrum and shows: Grade 2- 3 regressed follicles/hyaline vascular follicles or Grade 2- 3 plasmacytosis.
- KSHV/HHV8 LANA IHC- Negative
- Major criteria for further subclassification of iMCD-TAFRO (All 5 required)
- Anasarca (includes pleural effusions, ascites, subcutaneous edema)
- Thrombocytopenia (<1lac/cmm)
- Systemic inflammation: fever >37.5°C and/or CRP≧2mg/dL
- Organomegaly (CT scan): Small volume lymphadenopathy in >2 lymph node stations and/or Hepatomegaly and/or Splenomegaly
- Need at least 1 of the following:
- Bone marrow with reticulin fibrosis and/or megakaryocytic hyperplasia without another cause
- Renal insufficiency (pre-treatment; eGFR <60 ml/min/1.73m2, creatinine >1.3 mg/dL males >1.1mg/dL females) or renal failure (Dialysis)
- Exclusion criteria:
- Infections: EBV, HIV, KSHV/HHV8, COVID-19, tuberculosis etc
- Autoimmune disorders: SLE, rheumatoid arthritis, IgG4 related disease, Sjogren’s syndrome, HLH etc
- Malignancy: NHL, HL, myeloma, POEMS syndrome etc
KSHV/HHV8- Multicentric Castleman disease:
- Major criteria (All 3 required)
- Enlarged lymph nodes in at least 2 lymph node stations
- Microscopy consistent with Castleman disease spectrum and shows: Grade 2- 3 regressed follicles/hyaline vascular follicles or Grade 2- 3 plasmacytosis.
- KSHV/HHV8 LANA IHC- Positive plasmablasts
- Minor criteria (Need Fever and CRP>2gm/dL and at least 3 clinical/ laboratory criteria that are not related to other HIV infection complications)
- Laboratory criteria
- Hyponatremia
- Hypoalbuminemia
- Thrombocytopenia
- Anemia (including autoimmune hemolytic anemia)
- For flares (after original diagnosis): KSHV viral load
- Clinical criteria
- Splenomegaly
- Fatigue
- Weight loss
- Respiratory symptoms
- Gastrointestinal symptoms
- Neuropathy
- Headache
- Edema
- Rash
- Myalgia
- Fluid accumulation (edema, effusions)
- Laboratory criteria
- Exclusion criteria:
- Infections: EBV, COVID-19, tuberculosis etc
- Autoimmune disorders: SLE, rheumatoid arthritis etc
- Malignancy: KSHV/HHV8 negative NHL, HL, myeloma etc
Criteria for active disease:
- Fever
- Raised CRP levels- >20mg/L in absence of any other etiology
- At least 3 of the following other MCD related symptoms
- Peripheral lymphadenopathy
- Splenomegaly
- Edema
- Pleural effusion
- Ascites
- Cough
- Nasal obstruction
- Xerostomia
- Rash
- Central neurological symptoms
- Jaundice
- Autoimmune haemolytic anemia
Prognosis:
- 5 year overall survival rate
- Unicentric- 91%
- Multicentric- 65%
Pretreatment Work-up:
- History
- B-Symptoms
- ?Neuropathy (POEMS)
- Examination
- LN:
- Spleen:
- Active disease?
- WHO P. S.
- BSA
- IHC
- BMA and Bx
- CT (CAP)/ PET
- Hemoglobin
- TLC, DLC
- Platelet count
- LFT: Bili- T/D SGPT: SGOT:Albumin: Globulin:
- Creatinine
- Electrolytes: Na: K: Ca:Mg: PO4:
- Uric acid:
- LDH
- CRP
- ESR
- Ferritin
- HIV:
- HBsAg:
- HCV:
- HHV 8 DNA PCR
- EBV DNA PCR
- β2 microglobulin
- POEMS work up
- SPE:
- S.IFEP:
- SFLCA:
- Quant Ig:
- UPT
- ECHO(If anthracyclines planned)- LVEF- %
Treatment Plan:
May wait and watch for disease without any symptoms.
If severe systemic symptoms- Initial treatment with high dose parenteral steroids may be given.
About each modality of treatment:
- Siltuximab:
- Chimeric human- murine antibody against IL-6
- 11 mg/kg intravenously (IV) every 3 weeks
- Subsequently extended to 6-weekly maintenance
- More useful in reducing systemic symptoms, than reducing lymphadenopathy.
- Side effects: Cytopenia, hyperlipidemia
- R-CHOP
- CR rate is approximately 50%
- Median time for relapse- 6 months
- R- Thalidomide
- Rituximab is given weekly for 4 weeks
- Thalidomide is given for 3 months to 2 years
- 2 Year progression free survival- 60%
- Other drugs that are being used
- Tocilizumab-
- Antagonizes IL-6 receptor
- Especially useful in TAFRO
- 50 -100 mg IV weekly
- Tocilizumab-
Recent advances:
Characteristics of thrombocytopenia, anasarca, fever, reticulin fibrosis and organomegaly syndrome
TAFRO syndrome (thrombocytopenia, anasarca, fever, reticulin fibrosis and organomegaly) has emerged as a singular variant of iMCD in Asia and is associated with a severe course and a poor outcome. The present study describes the first large Western cohort of TAFRO syndrome patients (n = 25) meeting the All Japan TAFRO Syndrome Research Group diagnostic criteria.There were no significant differences between the two groups regarding treatment choice, response to rituximab (71% vs. 67%) or tocilizumab (69% vs. 91%) in TAFRO and iMCD-NOS, respectively.
https://doi.org/10.1111/bjh.17868
The disease course of Castleman disease patients with fatal outcomes in the ACCELERATE registry
To determine factors associated with mortality in Castleman disease, researchers analysed data from deceased patients in the ACCELERATE registry and compared them with matched controls. Of the 140 patients in ACCELERATE with a confirmed CD diagnosis, 10 had died. There was significantly decreased absolute lymphocyte count at months 3 and 6 in the deceased cohort compared with controls. There was a higher proportion of iMCD-TAFRO cases in the deceased group.
https://doi.org/10.1111/bjh.18214
Rituximab–bortezomib–dexamethasone induce high response rates in iMCD
A study designed a protocol using rituximab–bortezomib–dexamethasone (RVD) as first-line consolidation therapy for idiopathic multicentricCastleman disease (iMCD), a condition with limited treatment options. Five patients, including one with TAFRO syndrome, underwent the RVD regimen and achieved partial response (PR) or better. After four cycles, three patients achieved PR, and one achieved complete response. The patients discontinued treatment but remained stable for a median follow-up of 11 months, with a duration of response ranging from 7 to 13 months.
https://doi.org/10.1111/bjh.19000
Multidisciplinary approach in the diagnosis of Castleman disease
The study focused on diagnosing Castleman disease (CD), a rare group of hematological disorders, by applying clinical, pathological, and clonality testing criteria to 48 Italian patients with CD-like histological features. They confirmed CD in 60% of cases, including both unicentric and multicentric forms, with the latter further classified into subtypes. The study underscores the significance of a multidisciplinary approach for accurately diagnosing and treating CD-like reactive lymphadenitis, highlighting the necessity for collaboration between clinicians and pathologists.
https://doi.org/10.1111/bjh.19171
Sirolimus is effective for refractory/relapsed idiopathic multicentric Castleman disease
In a retrospective study of 26 patients with refractory/relapsed idiopathic multicentric Castleman disease (R/R iMCD), sirolimus treatment led to symptomatic and biochemical responses in 69.2% of patients, with a median time to partial remission of 1.9 months. The median follow-up time was 11.7 months, and the median time to next treatment was 46.2 months. No patients died during the study, and sirolimus was well tolerated with minimal adverse effects. These results suggest sirolimus is an effective and well-tolerated therapy for R/R iMCD.
https://doi.org/10.1007/s00277-024-05783-z
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.