
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
Large B Cell Lymphomas
This category includes following disorders:
- Diffuse large B-cell lymphoma, NOS
- T-cell/histiocyte-rich large B-cell lymphoma
- Diffuse large B-cell lymphoma / high grade B-cell lymphoma with MYC and BCL2 rearrangements
- ALK-positive large B-cell lymphoma
- Large B-cell lymphoma with IRF4 rearrangement
- High grade B-cell lymphoma with 11q aberrations
- Lymphomatoid granulomatosis
- EBV-positive diffuse large B-cell lymphoma
- Diffuse large B-cell lymphoma associated with chronic inflammation
- Fibrin-associated large B-cell lymphoma
- Fluid overload-associated large B-cell lymphoma
- Plasmablastic lymphoma
- Primary large B-cell lymphoma of immune-privileged sites (CNS, vitreo-retina, testes)
- Primary cutaneous diffuse large B-cell lymphoma, leg type
- Intravascular large B-cell lymphoma
- Primary mediastinal large B-cell lymphoma
- Mediastinal grey zone lymphoma
- High-grade B-cell lymphoma, NOS
Diffuse large B-cell lymphoma, NOS
Introduction:
- It is proliferation of large neoplastic B-lymphoid cells with diffuse growth pattern.
Epidemiology:
- Constitute 25-30% of adult NHL
- Median Age – 7th decade
- Male predominance
Etiology: Not known. Association is found with
- Genetic predisposition with immune dysregulation
- Herbicides
- Pesticides
- Dark hair dyes
- High BMI
- Tobacco use
- Alcohol use
- Inflammatory states
- Immunodeficiency with EBV infection
Pathogenesis:
Promoter substitution: Translocation between 3q27 (which contains BCL6) and chromosomal partner sites including 14q32 (IgH), 2p11 (Ig Kappa), and 22q11 (Ig Lambda)
↓
Over-expression of BCL6
↓
BCL6 promotes binding of several transcription factors to DNA and also induces germinal center associated functions
↓
Proliferation of lymphoid cells
Hans Classification/ algorithm based on gene expression profiles (Cell of origin):
- Germinal Centre B cell subtype:
- Have somatic hypermutations with mutations involving EZH2, GNA13, MEF2B, KMT2D, TNFRSF14, B2M and CREBBP genes
- CD10+ or BCL6+, IRF/MUM1- Negative.
- 5 year survival- 50-60%
- Activated B cell subtype:
- Associated with constitutive activation of the BCR signalling and the NFκB pathway
- Have mutations of genes of BCR signaling pathway such as MYD88, CD79B, PIM1 and PRDM1
- CD10- Negative, BCL6- Negative, IRF/MUM1+.
- 5 year survival- 15-30%
- Type 3 DLBCL- Not included in any of above 2
Clinical Features:
- Rapidly enlarging tumor mass
- Single/ multiple tumors
- Nodal involvement- Common
- Extranodal regions in 30-40% cases (Stomach, ileocecal region, salivary gland, thyroid, ocular adnexa, bone, liver, kidney and adrenal gland)
- B Symptoms- Seen in 30% patients
- Local compression- Vessels (SVC syndrome), airways etc
Investigations:
- Lymph node biopsy:
- Normal architecture completely distorted.
- Diffuse or vaguely nodular infiltration by medium-to large sized lymphoid cells
- Size of tumor cells is same or larger than nucleus of a macrophage/ twice the size of small lymphocyte
- High mitotic rate
- Tingible body macrophages may impart “starry sky” appearance
- Perinodal soft tissue is infiltrated
- Broad / fine bands of sclerosis may be observed
- Subtypes based on morphology of tumour cells
- Centroblastic – Median to large sized cells. Nucleus is oval / round, vesicular with fine chromatin and 2-4 membrane bound nucleoli. Cytoplasm is scanty and amphophilic to basophilic.
- Immunoblastic (MC malignancy arising in immunodeficiency). Nucleus has centrally located nucleolus and thick nuclear membrane. Cytoplasm is abundant and basophilic
- T cell / Histiocyte rich- Composed of T-cells and histiocytes. Large cells may resemble L & H cells centroblasts, immunoblasts or RS cells. Diffuse growth pattern is seen. Fine reticular fibrosis is present
- Anaplastic- Very large round, oval or polygonal cells. Nuclei are bizarre and pleomorphic. Cells may grow in cohesive pattern mimicking carcinoma or can have sinusoidal growth pattern
- Plasmablastic
- Cytoplasmic ALK positive
- Immunophenotyping
- Positive: Pan-B Markers (CD19, CD20, CD22, CD79a, PAX5-nuclear staining), Surface and/or cytoplasmic immunoglobulin (IgM>IgG>IgA), CD30 (Especially in anaplastic variants), BCL-2 (50% cases), Nuclear BCL-6 (60%-90% cases), LFA1 and CD44
- MYC and BCL2 protein over expression is seen in 20-30% patients and confers poor prognosis with 5 year survival with R-CHOP- <30%. (For diagnosis of double/ triple hit lymphoma, FISH for MYC, BCL-2 and BCL-6 rearrangements is needed). Those with double expression, must be submitted for FISH studies. Double hit lymphomas are GCB type, whereas double expressors are of ABC type.
- Other positive markers: Kappa/Lambda, cyclin D1, ALK, HHV8, SOX11
- Negative: CD25, CD56, CD103, BCL1, TdT, CD138, EBV-ISH
- Variable: CD10, CD23, CD30, CD43, CD5, IRF4/MUM1, p53 (Expression is not a good surrogate marker of p53 mutation)
- Denovo CD5+ DLBCL is diagnosed, when there is no history of CLL/SLL and in IHC/FISH tumor is negative for Cyclin D1 (expression of cyclin D1 indicates diagnosis of blastoid variant of mantle cell lymphoma)
- Proliferative index (Ki67)- High (Usually >80%)
- Immunoglobulin light and heavy chain rearrangements (mutations in variable region)
- Interphase cytogenetics/ FISH: Strongly recommended to exclude the diagnosis of diffuse large B cell lymphoma with MYC and BCL2 rearrangements
- FISH for MYC: MYC translocations partners are IG gene, BCL6, BCL11A, IKZF1, PAX5, RTFN1, CD96, SOCS1 and ZBTB5.
- If MYC is positive- BCL2 and BCL6 should be done to identify double hit lymphoma
- t (14 : 18) involving BCL-2 gene which is hallmark of follicular lymphoma is seen in 20-30% cases.
- 30% of abnormalities are associated with chromosome 3q27 involving BCL6 gene.
- Gene expression profiling: Gold standard test to identify cell of origin
- Bone marrow: Involved in 10-20% cases
Criteria for diagnosis:
Essential:
- Large B-cell lymphoma with diffuse or vaguely nodular growth pattern
- Mature B-cell phenotype
- Exclusion of other specific entities of large B-cell lymphoma
Desirable:
- Cell of origin subtyping
- Reporting of isolated MYC or dual MYC::BCL6 translocations
- Genetic testing, if relevant for clinical decision making
Prognosis:
- Aggressive but potentially curable with chemotherapy
- 10-15% have primary refractory disease
- 20-30% patients relapse after treatment.
- Overall 5 year survival with R-CHOP is approximately 75%
- Intenational Prognostic Index (IPI): Factors included are:
- Age >60 years
- Raised LDH
- Performance status- 2-4
- Stage III or IV
- Extranodal disease >1 site
Risk category | Score | 5 year survival | 5 year survival |
Low | 0 or 1 | 69-83% | 51-73% |
Low- Intermediate | 2 | 46% | 43% |
High Intermediate | 3 | 32% | 26% |
High | 4 or 5 | Less | Less |
- Prognostic markers to assess risk of CNS disease: Factors included
- Age >60 years
- Raised S. LDH levels
- PS- >1
- Stage III or IV
- Extranodal involvement- >1 site
Risk category | Score |
Low | 0-1 |
Intermediate | 2- 3 |
High |
- 70-80% of CNS relapses involve brain parenchyma, rest involve leptomeninges.
- In 45% patients, CNS relapse is associated with systemic relapse
- Poor prognostic markers
- High proliferative rate
- Expression of BCL 2, XCAP, IRF/MUM1, Cyclin D2, Cyclin D3, P53, CD5, FOXP1, PKC-Beta, ICAM1, HLADR, c-FLIP, Survivin
- Immunoblastic/ Centroblastic variants
- Elevated LDH
- High beta 2 microglobulin levels
- Mutation of p53 gene
- MYC rearrangements especially with IG gene as partner
- Bulky disease
- Age >60 years
- ECOG Performance score- 2 or more
- Advanced stage disease
- High IPI index
- High risk molecular subgroups: Double hit signature positive and molecular high grade types
- Factors associated with good prognosis
- Germinal centre B-like DLBCL
- BCL 6 translocation and expression
- Expression of CD10, LMO2
- Expression of MHC class II genes
- Infiltration of CD4+ cells
Lymphomas which are treated similar to DLBCL:
- DLBCL co-existing with follicular lymphoma/ MALT lymphoma
- Follicular lymphoma- Grade 3
- Intravascular large B cell lymphoma
- DLBCL associated with chronic inflammation
- ALK Positive DLBCL
- EBV Positive DLBCL
- DLBCL with IRF4/MUM1 rearrangement
Subtypes which are not treated like DLBCL:
- Primary DLBCL of CNS
- Primary retinal large cell lymphoma
- Double/ triple hit lymphoma
- High grade B cell lymphoma -NOS
- Primary cutaneous DLBCL- Leg type
- T Cell/ Histiocyte rich DLBCL
- DLBCL arising from CLL (Ritcher transformation)
Pretreatment Work-up:
- History
- B-Symptoms
- Examination
- LN:
- Spleen:
- WHO P. S.
- BSA
- IHC
- BMA and Bx (Not needed if PET –negative)
- Whole body PET-CT
- Bulky disease (>7.5cm)
- Stage
- Hemoglobin
- TLC, DLC
- Platelet count
- LFT: Bili- T/D SGPT: SGOT: Albumin: Globulin:
- Creatinine
- Electrolytes: Na: K: Ca: Mg: PO4:
- Uric acid:
- LDH
- β2 Microglobulin
- HIV:
- HBsAg:
- HCV:
- UPT
- Cytogenetics
- CSF (if 4-6 risk factors, HIV Lymphoma, Testicular and double expressor)
- FISH- MYC, BCL1, BCL6 (For double expressors)
- IPI-Prognostic score
- ECHO (If anthracyclines planned) LVEF- %
- Chemotherapy consent after informing about disease, prognosis, cost of therapy, side effects, hygiene, food and contraception
- Fertility preservation
- PICC line insertion and Chest X ray after line insertion
- Tumor board meeting and decision
- Attach supportive care drug sheet
- Inform primary care physician
Treatment Plan:
Paediatric DLBCL: Refer to R-LMB Intergroup B NHL 2010 trial protocol in NHL Section. Click here
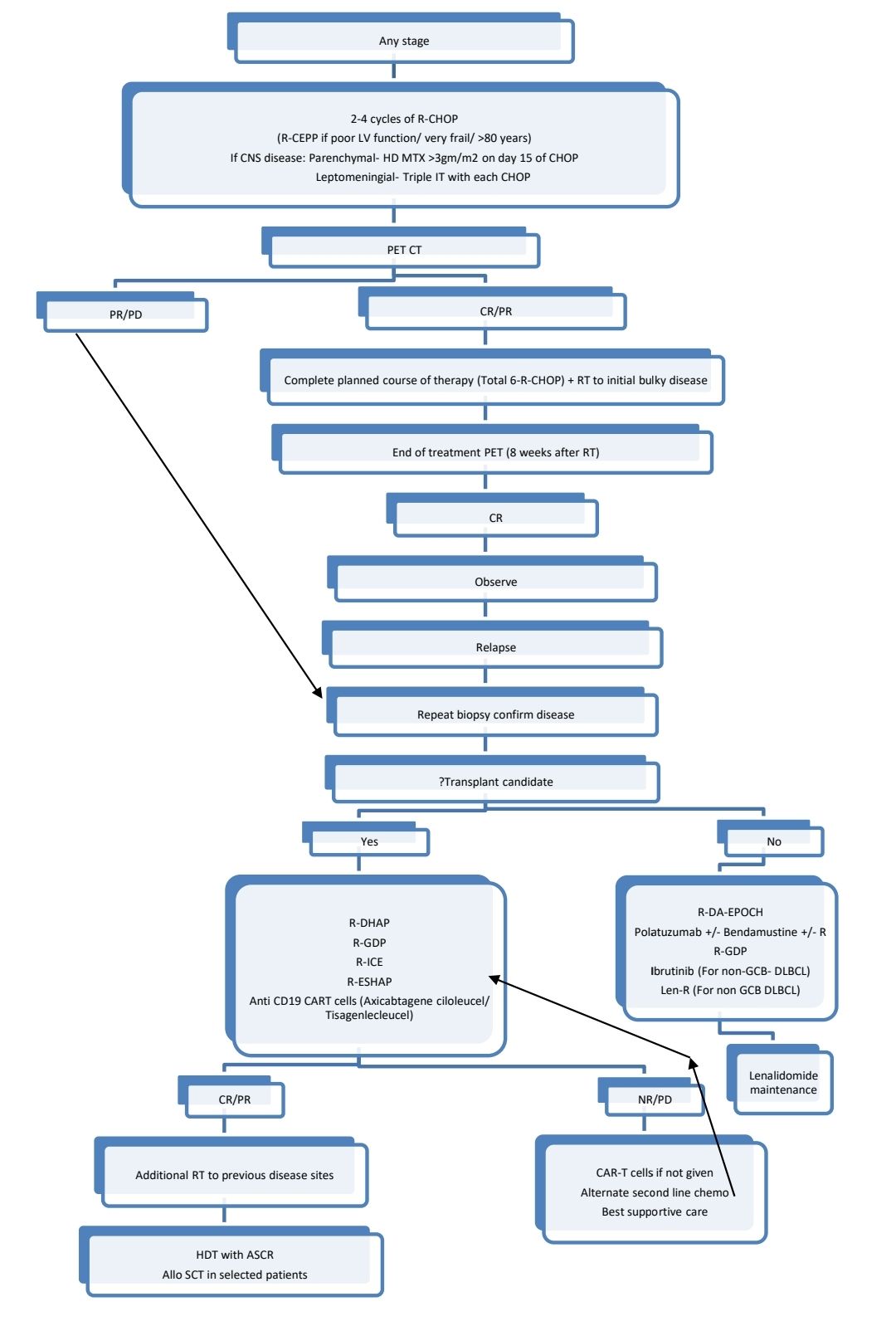
CNS Prophylaxis:
- IT- Methotrexate- 12mg- Day 1 of each cycle (Although many studies have shown that only intrathecal chemo will not give adequate protection against CNS relapse).
- Methotrexate- 3gm/m2- over 2 to 4hrs followed by Folinic acid rescue, 2-3 cycles 14 days apart after completion of 6 cycles of chemotherapy. This is expected to protect against parenchymal relapse. Alternatively, HD MTX may be given on Day 10 of alternating cycles of R-CHOP (which is known as intercalated HD-MTX)
- CNS prophylaxis must be given to following patients
- High risk of CNS disease
- 3 or more extranodal disease
- HIV associated lymphoma
- Testicular involvement
- High grade B cell lymphomas
- Double/ triple hit lymphomas
- Primary cutaneous DLBCL- Leg type
- Intravascular large B cell lymphoma
- DLBCL involving breast/ uterus/ kidney/ adrenals/ paranasal sinuses/ Epidural space/ orbit/ Bone
- If there is concurrent CNS disease:
- Parenchymal: Methotrexate- 3gm/m2 given on day 15 of 21 days R-CHOP cycle, that has been supported by growth factors
- Leptomeningeal: Triple IT on days 1 and 15 of each cycle/ Consider Ommaya reservivor treatment +/- Methotrexate -3gm/m2
Options for relapsed disease after HDT with ASCR/ Multiple refractory disease:
- Polatuzumab-Rituximab-Cyclo-Doxo-Pred
- Anti CD19 CAR T-cell therapy- Axicabtagene ciloleucel, Lisocabtagene maraleucel, Tisagenlecleucel
- Brentuximab vedotin for CD30+ disease
- Ibrutinib (non-germinal center B-cell–like DLBCL)
- Lenalidomide ± rituximab (non-GCB DLBCL)
- Bispecific T-cell engager therapy- Epcoritamab-bysp, Glofitamab-gxbm
- Non T cell mediated therapy- Loncastuximab tesirine-lpyl, Selinexor
- Salvage therapy followed by Allogeneic SCT
Indications for radiotherapy:
- Initial bulky disease- 36 Gy IFRT
- Testicular lymphoma- After completion of chemotherapy, scrotal RT is given (25-30 Gy)
- Isolated skeletal sites
Monitoring After Treatment/ Follow-up:
- History, examination and labs every 3-6 months for 5 years and then yearly/ as clinically indicated
- CT (C/A/P) with contrast every 6 monthly for 2 years and then only if clinically indicated
Special Situations:
- DLBCL with pregnancy:
- 1st trimester: Therapeutic abortion should be considered
- 2nd and 3rd trimester: CHOP can be administered relatively safely
- Prognosis of who receive optimal therapy is same as non-pregnant patients
- DLBCL in elderly, frail or unfit patients
- Biological age is more important than chronological age. Fit patient with normal performance score may be treated like any other DLBCL patient.
- Steroid pretreatment often renders them suitable for standard R-CHOP
- Primary G-CSF prophylaxis must be given
- Etoposide can be replaced for Doxorubicn or dose of Doxorubicin may be decreased as per the protocol.
- R-GVP (Rituximab, Gemcitabine, Vincristine and Prednisolone) is the alternate option.
T-cell/histiocyte-rich large B-cell lymphoma
- Characterized by <10% large, atypical B cells embedded in a background of abundant T cells (Positive for CD3 and CD5) and frequently histiocytes (Positive for CD68)
- Both NLPHL and T-cell/histiocyte-rich large B-cell lymphoma harbour mutations affecting JUNB, DUSP2, SGK1, SOCS1 and CREBBP genes
- Seen usually in middle aged men.
- Accounts for <10% of DLBCL
- Present with fever, malaise and hepatosplenomegaly
- Aggressive disease
- Relatively poor prognosis
- 5 year OS- 50%
- Treatment- 4 cycles of R-CHOP-14 followed by 3 cycles of R-ICE.
Diffuse large B-cell lymphoma / high grade B-cell lymphoma with MYC and BCL2 rearrangements
(Double Hit Lymphoma)
- High grade B cell lymphomas with translocations of MYC and (BCL2 and/or BCL6) as detected by FISH or standard cytogenetics.
- Most of them are germinal center B cell like expression.
- Pathogenesis:
- Translocation of BCL2 (Chr. 18q21) to IGH (Chr. 14q32)à Aberrant BCL2 expression à Increased apoptotic resistance
- Translocation of MYC (Chr. 8q24) to IGH (Chr. 14q32)à MYC activation à Increased proliferation
- Several other translocation partners are also seen.
- Represents 8% of all DLBCL cases
- 3 subtypes:
- Without BCL6 rearrangement
- With BCL6 rearrangement
- With TdT expression
- Morphology: Similar to DLBCL. Some have Burkitt's lymphoma like morphology. Some can have blastoid morphology resembling lymphoblasts.
- Immunohistochemisrty: Positive for
- Pan B-cell antigens: CD19, CD20, CD79a and PAX5.
- CD10 (88%-98%), BCL6 (75%-89%) and MUM1/IRF4 (17%-42%). Hence, 91%-99% of these tumours have GCB-like phenotype.
- MYC (78%-86%), BCL2 proteins (90% to 95%) and double-expressors (71-81%)
- Ki67/MIB1 proliferation index is high (50-100%)
- Sequential strategy for FISH testing (This strategy must be applied for all cases of DLBCL, irrespective of IHC findings. If MYC expression on IHC is moderate to strong and expressed in >70% cells, then chances of MYC rearrangements being positive is high)): Testing with MYC FISH probeà If MYC is rearranged, then following must be tested
- BCL2 (and BCL6) rearrangement status
- MYC translocation partner
- Present often with poor prognostic parameters such as
- Advanced stage
- Elevated LDH
- BM involvement
- CNS involvement
- Advanced age
- Prognosis: Aggressive clinical course. With R-CHOP alone, 5 year OS is 40-50%.
- Treatment:
- DA-EPOCH- 6 cycles (Other options include- R-HyperCVAD, R-CODOX-M/IVAC). Outcome with R-CHOP is very poor.
- Consolidative ISRT is preferred for localised disease
- Consolidation with HDT with ASCR - Role is not clear. Avoid if patient is not fit for the procedure.
- CNS prophylaxis has to be given
ALK-positive large B-cell lymphoma
- Very rare- Less than 1% of all DLBCL
- Tumor cells have plasmablastic immunophenotype
- Less than 200 cases reported so far
- Translocations involving ALK at chromosome 2p23 (Most common is t(2;17) involing clathrin)à Constitutive activation of ALK tyrosine kinase.
- Commonly affects cervical lymph nodes
- Sinusoidal growth pattern of large immunoblast like cells
- IHC- Positive for ALK, EMA, BOB.1, OCT-2, CD45RB, cytoplasmic immunoglobulin (IgA>IgG; lambda>kappa), MYC, STAT3, plasma cell markers (CD138, CD38, MUM1, VS38c, BLIMP1 and XBP1.)
- Poor prognosis with median survival of 11 months
- No optimal treatment established
- Usually CD20 Negative. Hence Rituximab is not necessary
- First line chemotherapies:
- Elderly patients: DA-EPOCH, CHOEP and Mini-CHOP (frail or elderly patients)
- For fit patients: HyperCVAD, CODOX-M/IVAC
- Second line: Platinum based regimens followed by HDT/ASCR, Next generation ALK inhibitors (alectinib and lorlatinib)
- First line chemotherapies:
Large B-cell lymphoma with IRF4 rearrangement
- Large B cell lymphoma with follicular and/or diffuse growth pattern defined by strong expression of IRF4 (MUM1) usually due to an IG::IRF4 translocation
- Commonly affects Waldeyer’s ring (especially tonsils) and cervical lymph nodes
- Rare disease and mostly seen in children
- Pathogenesis: A structural variant juxtaposes the IRF4 gene next to an IG locus, leading to pathognomonic overexpression of IRF4 (MUM1).
- Morphology: Sheets of atypical centroblasts arranged in 3 patterns
- Purely follicular
- Purely diffuse
- Combined follicular and diffuse
- Immunohistochemistry: Positive for IRF4/MUM1, BCL6, CD10 and BCL2
- Molecular test for IRF4 translocation is positive (Usually IG::IRF4 translocation)
- Prognosis: Favorable
High grade B-cell lymphoma with 11q aberrations
(Burkitt like lymphoma with 11q aberration)
- Large B cell lymphoma with chromosome 11q-gain/loss
- Sites: Head and neck lymph nodes (60%), GIT (30%)
- Very rare disease
- Pathogenesis is not clear, but genes involved include KMT2A, ETS1 and GNA13.
- Microscopy: Similar to Burkitt lymphoma
- IHC:
- Positive- B-lineage markers, CD10 and BCL6, a high proliferation index (Ki67≥90%)
- Negative- BCL2
- MYC may be positive even though MYC rearrangement is not seen
- Flow cytometry: Expression of CD16, Cd56 and CD8 is highly characteristic
- Interphase FISH: can detect 11q abnormality
- Prognosis: Good. Recurrences are rarely seen.
- Treatment: Similar to Burkitt’s lymphoma
Lymphomatoid granulomatosis
- It is an angiocentric and angiodestructive lymphoproliferative disease involving extranodal sites comprised of EBV positive B cells admixed with reactive T-cells, which usually numerically predominate.
- Commonly involves lung.
- Common in children
- M:F= 2:1
- Etiology:Predisposing factors
- Allogeneic organ transplantation
- Wiskott Aldrich syndrome
- HIV infections
- X-linked lymphoproliferative syndrome
- Pathogenesis: Defective response to EBV infection by CD8+ cytotoxic T cells à Diminished immune control of EBV infected B cells
- Present with cough, dyspnea, chest pain, fever, malaise, and weight loss
- Biopsy of pulmonary nodule
- Angiocentric and angiodestructive polymorphous lymphoid infiltrate
- Lymphocytes predominate
- Admixed plasma cell, immunoblasts, histiocytes seen
- Multinucleated cells may be seen
- Central necrosis is oftenseen
- No well-formed granulomas in lung lesions, but may be found in skin lesions
- Vascular changes- Lymphocytic vasculitis
- Grading:
- Grade I- Polymorphous lymphoid infiltrate without cytological atypia. FISH with EBER1/2 probe shows EBV positive cells < 5 / HPF
- Grade II- Contain occasional large lymphoid cells or immunoblasts in polymorphous background. Necrosis is common. EBV positive cells – 5-50/HPF
- Grade III- Readily identified as malignant lymphoma. Marked pleomorphism and necrosis. EBV positive cells > 50 / HPF
- Immunophenotyping (atypical large B cells)
- Positive – CD20, CD79a, CD30 (variable), LMP1
- Negative – CD15
- ISH using EBER probe: Useful in identifying EBV positive cells
- EBV genome identified by southern blotting
- Prognosis:
- Waxing and waning clinical course with rare spontaneous remissions
- Median survival - < 2 years
- Treatment:
- Grade I & II treatment with INF alfa 2b
- Others: R-DA-EPOCH
EBV-positive diffuse large B-cell lymphoma
- Large B cell lymphoma with the majority of the neoplastic cells harbouring EBV
- Following must be excluded before making diagnosis
- Lymphomatoid granulomatosis
- Infectious mononucleosis
- NHLs- Plasmablastic lymphoma, primary effusion lymphoma, DLBCL associated with chronic inflammation
- Epidemiology
- Accounts for 8-10% of DLBCLs in asians
- Median age- 71 years
- M:F= 1.4:1
- Sites involved
- 70%- Extranodal disease (Skin, lung, Tonsils, Stomach)
- 30%- Lymph node alone
- Morphology:
- Architecture of involved tissue is altered
- Large transformed cells/ immunoblasts
- RS like giant cells are present
- Variable amount of reactive component- Small lymphocytes, plasma cells, histiocytes, epithelioid cells
- IHC- Same as DLBCL
- Prognosis
- Aggressive disease
- Median survival- 2 years
- Treatment- Same as DLBCL
Diffuse large B-cell lymphoma associated with chronic inflammation
- It is EBV associated large B cell lymphoma occurring in the setting of longstanding chronic inflammation involving confined natural body spaces
- Epidemiology:
- Median age- 70 years
- M:F= 12.3 :1
- Etiology
- Artificial pneumothorax, which was used as treatment for TB
- Chronic pyothorax
- EBV
- Chronic osteomyelitis
- Morphology, IHC- Similar to DLBCL
- Prognosis
- Aggressive lymphoma
- 5 year OS- 20-35%
- Treatment- Complete surgical excision followed by chemotherapy
Fibrin-associated large B-cell lymphoma
- Large B cell lymphoma found incidentally at sites of chronic fibrin deposition in confined anatomic spaces
- Anatomical spaces include cyst and pseudocyst cavities in:
- Peri-implant space of breast implants
- Chronic haematomas
- Intravascular or intracardiac locations, such as the surface of cardiac myxomas, endovascular grafts and prosthetic cardiac valves
- Mostly asymptomatic
- Often EBV associated
- Microscopy: Large atypical lymphoid cells surrounded by fibrin and cellular debris
- Infiltration into adjacent tissue is absent
- IHC: Similar to DLBCL
- After excision, no subsequent lymphoma is seen. Hence, no active treatment is necessary.
Fluid overload-associated large B-cell lymphoma
- Large B cell lymphoma presenting as serous effusions without detectable tumour masses, often in patients with fluid overload states
- Not associated with KSHV/ HHV8
- Mostly seen in pleural cavity
- Underlying disorders include:
- Chronic heart failure
- Renal insufficiency
- Protein losing enteropathy
- Liver failure/cirrhosis
- Very rare: <100 cases reported so far
- Rarely associated with HIV
- Prognosis: Favorable
- Treatment: R-CHOP chemotherapy
Plasmablastic lymphoma
- Aggressive lymphoid neoplasm of large atypical Bcells with plasmablastic or immunoblastic morphology.
- Microscopy: Diffuse and cohesive proliferation of cells resembling immunoblasts with frequent mitosis are seen. Apoptosis and tangible body macrophages are present.
- Mostly extranodal disease with 50% cases occurring in nasal/ oral cavity
- Commonly seen in patients with immunodeficiency especially HIV, organ/ stem cell transplantation and patients undergoing CAR T cell therapy.
- Always associated with EBV infection
- IHC:
- Positive: Plasma cell markers (CD138, CD38, VS38c, Blimp1, XBP1), CD79a (50-85% patients), IRF4 (MUM1), MYC, EMA, CD30 (30% cases), Cytoplasmic immunoglobulin (60% patients), light chain restriction is noted
- Negative: CD45, CD20, PAX5, CD56
- Ki67- Very high
- EBV EBER in situ hybdridization- Positive
- Prognosis- Poor
Primary large B-cell lymphoma of immune-privileged sites
(CNS, vitreo-retina, testes)
Primary testicular lymphoma
- Accounts for 1-2% of all lymphomas
- Incidence- 0.26/1lac men/ year
- Morphology- 80-90% are DLBCL
- 6% have bilateral involvement
- Most present in stage I or II
- Has tendency to spread to extra-nodal sites such as contralateral testis, CNS, skin, Waldeyer's ring, lung, pleura, soft tissues
- Median survival- 4.4 years
- Treatment:
- Orchiectomy followed by 6 cycles of R-CHOP
- CNS prophylaxis has to be given
- Radiation to contralateral testis after 6 R-CHOP
Primary CNS Lymphoma- Discussed separately in Miscellaneous diseases section
Primary cutaneous diffuse large B-cell lymphoma, leg type
- Epidemiology:
- 4% of all cutaneous NHL
- 20% of all cutaneous B cell lymphomas
- Median age- 70 years
- M:F- 1:3
- Presents as red/bluish red tumor
- Prognosis: 5 year survival- 50%
- Treatment-
- Localised, single lesion- ISRT
- Involvement of lymph nodes/ multiple lesions/ Relapse after ISRT- 6 cycles of R-CHOP followed by Local ISRT
- Relapse/ refractory cases are treated like relapsed/ refractory DLBCL.
- Should receive CNS prophylaxis
Intravascular large B-cell lymphoma
- Rare subtype of extranodal DLBCL characterized by presence of lymphoma cells only in the lumina of small vessels
- Epidemiology:
- Median age- 76 years
- M:F= 1.1:1
- Presents as 3 patterns
- Classic subtype:
- Asian pattern: Fever, pain, organ related symptoms, multi-organ failure, hepatosplenomegaly, pancytopenia
- Western pattern: Neurological – Dementia, focal neurological symptoms
- Cutaneous subtype: Tumor limited to skin (plaque or nodule)
- Hemophagocytic subtype
- Classic subtype:
- Pathogenesis: Defect in homing receptors on the neoplastic cells – CD29 (β1 integrin) & CD54 (ICAM-1)
- Morphology
- Neoplastic lymphoid cells are mainly lodged in the lumina of small vessels in many organs.
- Tumor cells are large with vesicular nuclei with prominent nucleoli
- Frequent mitotic figures seen
- Immunophenotyping: Positive- B – cell associated antigens , CD5, PDL1, IRF4 (MUM4)
- Investigations:
- S. LDH- Elevated
- Beta 2 microglobulin- Raised
- ESR- Raised
- LFT, RFT- May be deranged
- Prognosis - Extremely aggressive, responds poorly to chemotherapy
- Treatment:
- R-CHOP with CNS prophylaxis
- If CNS is involved- Intense chemotherapy that contain high dose methotrexate and cytarabine
Primary mediastinal large B-cell lymphoma
- It is a subtype of diffuse large B-cell lymphoma arising in mediastinum of putative thymic B-cell origin.
- Involves dysregulation of JAK-STAT and NF-kB pathways
- Epidemiology:
- Median age- 35 years
- Slight female predominance (1:2)
- 2-4% of all NHL
- Clinical features
- Bulky anterior mediastinal mass with invasion of local structures
- SVC syndrome
- Pleural effusion
- Lymph node biopsy:
- Similar to DLBCL- Neoplastic cells vary in size and nuclear shape and have abundant pale cytoplasm
- Diffuse proliferation
- Dense fibrosis forming compartments
- Thymic remnants can be identified by IHC
- Immunophenotyping
- Positive – B cells markers (CD19, 20, 22, 79a), CD30, IRF4/MUM1, Leukocyte common antigen (CD45)
- Negative- HLA – class I & II, CD10, CD5, CD21, CD15
- Variable- BCL2, BCL6
- Cytogenetics:
- Hyperdiploid 9p, involving JAK 2
- Gain in Chromosome 2p15, involving C-REL
- Loss of 1p, 3p, 13q, 15q, 17q
- Gene expression profile- More like classical Hodgkin’s disease, rather than DLBCL
- Prognosis – Response to therapy is good
- Pretreatment work up is similar to DLCBCL
- Treatment:
- R- DA- EPOCH for 6 cycles +/- ISRT
- CNS prophylaxis- Similar to DCLBL
- For persistent focal disease RT is added.
- Treatment of Refractory or relapsed disease (Biopsy must be performed at the time of relapse)
- Treat like relapse/refractory DLBCL.
- Consider RT alone, for localized disease and if RT was not used earlier.
- Pembrolizumab
- Nivolumab +/- Brentuximab
- CAR-T cell therapy
Mediastinal grey zone lymphoma
- It is B-cell lymphoma with features intermediate between primary mediatsinal B cell lymphoma and classical Hodgkin's lymphoma
- Present with large anterior mediastinal mass with or without supraclavicular lymph nodes
- Commonly seen in young adults, common in men
- Morphology:
- Pleomorphic cells in a diffusely fibrous stroma.
- Necrosis without neutrophilic infiltration is common
- IHC:
- Positive: CD45, CD30, CD15, CD20, CD79A, PAX5, BOB1, OCT2
- Negative: EBV,
- Variable: BCL6, CD10, ALK
- Prognosis: Worse compared to DLBCL or HL
- Treated like Primary mediastinal B cell lymphoma
Large B cell lymphoma arising in HHV8 associated multicentric Castleman's disease
- It is composed of monoclonal proliferation of HHV8 infected lymphoid cells, resembling plasmablasts expressing IgM.
- It is usually seen in HIV infected patients
- Presents with lymphadenopathy, massive splenomegaly
- Often associated with Kaposi's sarcoma
- Highly aggressive tumor with median survival of only few months
B Cell Lymphoma- Unclassifiable- with features intermediate between DLBCL and Burkitt's Lymphoma
- Morphology and genetic features of both DLBCL and Burkitt lymphoma
- Heterogenous category and is not considered a distinct entity
- Burkitt lymphoma like morphology with BCL2 positivity
- Aggressive clinical course
- Should be treated like Burkitt lymphoma
Recent advances:
CNS Prophylaxis in DLBCL
In a study by Orellana Noia et al patients with DLBCL treated with DA-EPOCH-R with IT-MTX as CNS prophylaxis were compared with those treated with R-CHOP with IV-HD-MTX. CNS relapse rates were not significantly different in these groups (5.4% Vs 6.8%). Relapse rates in patients treated with R-ACVBP (Rituximab, doxorubicin, cyclophosphamide, vindesine, bleomycin and prednisolone) with IT-MTX followed by consolidative CNS prophylaxis with IV-MTX, rituximab, ifosfamide, etoposide and cytosine was very low (1.6%).
https://doi.org/10.1182/Blood.2021012888
Tisagenlecleucel in relapsed/refractory Aggressive B cell Lymphomas
Tisagenlecleucel is anti CD-19 CAR-T cell therapy approved for DLBCL who have failed at least two lines of therapy. This therapy was evaluated in patients who were refractory disease or disease that progressed within 12 months after 1st line of therapy. Standard care group patients received ASCT. Study involved 322 patients who underwent randomization. At 6 weeks, lymphoma progression was higher in Tisagenlecleucel group compared to standard-care group (25% Vs 13%). Incidence of adverse effects was same in both groups.
https://doi.org/10.1056/NEJMoa2116596
Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma
In a recent study axicabtageneciloleucel (an autologous anti-CD19 chimeric antigen receptor T-cell therapy) was compared with standard care (Salvage therapy followed by ASCT) in patients with early relapse of high grade B cell lymphoma. Approximately 180 patients were assigned to each arm. The 24 month event free survival was 41% in study group compared to standard care group. 83% patients in study group showed response, compared to 50% in standard care group.
https://doi.org/10.1056/NEJMoa2116133
Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma
Only 60% patients with DLBCL are cured by R-CHOP chemotherapy. Polatuzumab vedotin (antiCD79a antibody) was used as replacement to vincristine in a recent phase 3 trial. Survival at a median follow up of 28 months was significantly higher in Polatuzumab group compared to R-CHOP group (76% Vs 70%). Safety profile was similar in both groups.
https://doi.org/10.1056/NEJMoa2115304
Brentuximab and lenalidomide in refractory DLBCL
37 patients who were not eligible for stem cell transplant/ CART cell therapy were included in this study. BV was given once in 21 days and Len was given continuously for maximum of 16 cycles. This regimen was well tolerated, with major side effect being neutropenia. Overall response rate was 57% with median duration of response being 13 months. As expected, highest response was seen in patients with CD30+ DLBCL.
https://doi.org/10.1182/blood.2021011894
The antibody-drug conjugate loncastuximabtesirine for the treatment of diffuse large B-cell lymphoma
Loncastuximabtesirine is a CD19-targeting antibody-drug conjugate approved by the US Food and Drug Administration for relapsed DLBCL after 2 lines of systemic therapy based on a trial showing a 48.3% overall response rate. The spectrum of its clinical applications is expanding and is now being tested in other B-cell malignancies.
https://doi.org/10.1182/blood.2021014663
New Dynamic Prognostic Index for Diffuse Large B-Cell Lymphoma: International Metabolic Prognostic Index
Baseline metabolic tumor volume (MTV) is a promising biomarker in diffuse large B-cell lymphoma (DLBCL). This study was conducted to determine the best statistical relationship between MTV and survival and to compare MTV with the International Prognostic Index. It was found that MTV was a better predictor than IPI for PFS and OS. A new prognostic index has been proposed using MTV, age, and stage, which outperforms IPI and enables individualized estimates of patient outcome.
https://doi.org/10.1200/JCO.21.02063
Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma
Glofitamab (a T-cell-engaging bispecific antibody) was tested in relapsed DLBCL.Patients received pretreatment with obinutuzumab to mitigate cytokine release syndrome, followed by fixed-duration glofitamab monotherapy (12 cycles total). At a median follow-up of 12.6 months, 39% of the patients had a complete response. The median time to a complete response was 42 days. The majority (78%) of complete responses were ongoing at 12 months. Discontinuation of glofitamab due to adverse events occurred in 9% of the patients.
https://doi.org/10.1056/NEJMoa2206913
Rituximab, Lenalidomide, and Ibrutinib in DLBCL
Present study enrolled 60 patients with newly diagnosed non–germinal center B-cell-like DLBCL. Patients were treated with rituximab 375 mg/m2 intravenous once on day 1, lenalidomide 25 mg once per day on days 1-10, and ibrutinib 560 mg once daily continuously of each 21-day cycle. After two cycles, standard chemotherapy was added to RLI for six additional cycles. The revised international prognostic index identified 42% as high risk, and 62% were double expressor of MYC and BCL2 protein. The ORR after two cycles of RLI was 86.2%, and the complete response rate at the end of RLI-chemotherapy was 94.5%. With a median follow-up of 31 months, the progression-free survival and overall survival were at 91.3% and 96.6% at 2 years, respectively.
https://doi.org/10.1200/JCO.22.00597
Next-generation ALK inhibitors are highly active in ALK-positive large B-cell lymphoma
Anecdotal reports of the first-generation ALKicrizotinib with cytotoxic chemotherapy in ALK-LBCL have been discouraging. Alectinib and lorlatinib are next-generation ALK inhibitors with higher potency than crizotinib and are effective in crizotinib-refractory ALK-positive cancers. Patient-derived xenograft (PDX) models of ALK-LBCL were used in present study. Upon engraftment, mice were assigned to tumor volume-matched groups and dosed daily with lorlatinib, alectinib, crizotinib, or vehicle (acidified water) by oral gavage. Tumor volume was measured daily thereafter.
Study suggested to check whether adding alectinib/lorlatinib to first-line chemotherapy improves outcomes,
https://doi.org/10.1182/blood.2022015443
New Dynamic Prognostic Index for Diffuse Large B-Cell Lymphoma: International Metabolic Prognostic Index
Baseline metabolic tumor volume (MTV) is a promising biomarker in diffuse large B-cell lymphoma (DLBCL). This study was conducted to determine the best statistical relationship between MTV and survival and to compare MTV with the International Prognostic Index. It was found that MTV was a better predictor than IPI for PFS and OS. A new prognostic index has been proposed using MTV, age, and stage, which outperforms IPI and enables individualized estimates of patient outcome.
https://doi.org/10.1200/JCO.21.02063
Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma
Glofitamab (a T-cell-engaging bispecific antibody) was tested in relapsed DLBCL.Patients received pretreatment with obinutuzumab to mitigate cytokine release syndrome, followed by fixed-duration glofitamab monotherapy (12 cycles total). At a median follow-up of 12.6 months, 39% of the patients had a complete response. The median time to a complete response was 42 days. The majority (78%) of complete responses were ongoing at 12 months. Discontinuation of glofitamab due to adverse events occurred in 9% of the patients.
https://doi.org/10.1056/NEJMoa2206913
Pembrolizumab in relapsed or refractory primary mediastinal large B-cell lymphoma
The final analysis of the KEYNOTE-170 study assessed the long-term efficacy and safety of pembrolizumab in relapsed/refractory primary mediastinal B-cell lymphoma (PMBCL) patients. With a median follow-up of 48.7 months, pembrolizumab demonstrated an objective response rate of 41.5%, including a complete response rate of 20.8%. The median duration of response was not reached, and patients who achieved a complete response did not experience disease progression. The median progression-free survival was 4.3 months, and the 4-year overall survival rate was 45.3%. Treatment-related adverse events were observed in 56.6% of patients, with most being of low to moderate severity.
https://doi.org/10.1182/blood.2022019340
Lenalidomide plus rituximab for the initial treatment of frail older patients with DLBCL
The FIL_ReRi study, a two-stage single-arm trial, explored the efficacy and safety of a chemo-free combination of rituximab and lenalidomide (R2) in untreated, frail diffuse large B-cell lymphoma (DLBCL) patients aged 70 or older. With a 50.8% overall response rate and a 27.7% complete response rate after six cycles, the R2 combination demonstrated activity in a substantial portion of subjects. While the median progression-free survival was 14 months, and the 2-year duration of response was 64%, further investigation is warranted for this chemo-free approach in frail older DLBCL patients.
https://doi.org/10.1182/blood.2022019173
Comparison of standardized prophylactic high-dose and intrathecal methotrexate for DLBCL with a high risk of CNS relapse
In a multicenter retrospective study, the prophylactic effects of high-dose methotrexate (HD-MTX) and intrathecal methotrexate (IT-MTX) were compared in 132 patients with high-risk diffuse large B-cell lymphoma (DLBCL). The patients received frontline chemotherapy and either HD-MTX (2014–2020, n = 98) or IT-MTX (2003–2013, n = 34). After a median follow-up of 52 months, 11 patients had isolated CNS relapse (6 in the HD-MTX group and 5 in the IT-MTX group). The cumulative incidence of CNS relapse at 3 years was 3.9% in the HD-MTX group and 6.1% in the IT-MTX group. The study found that HD-MTX was not superior to IT-MTX in preventing CNS relapse in high-risk DLBCL.
https://doi.org/10.1007/s12185-023-03700-0
Tafasitamab for patients with relapsed or refractory diffuse large B-cell lymphoma
Tafasitamab is a humanized, CD19-directed cytolytic monoclonal antibody. The final 5-year analysis of the L-MIND study evaluated tafasitamab and lenalidomide in autologous stem cell transplant-ineligible relapsed/refractory DLBCL patients. Results showed a 57.5% objective response rate with a 41.3% complete response rate, and a median progression-free survival of 11.6 months. Patients who received one prior line of therapy demonstrated higher response rates compared to those with two or more prior lines.
https://doi.org/10.3324/haematol.2023.283480
Pembrolizumab plus vorinostat in relapsed/refractory B-cell non-Hodgkin lymphoma
The study aimed to assess the safety and preliminary efficacy of pembrolizumab with vorinostat in relapsed/refractory B-cell lymphomas, given the disappointing outcomes with programmed death-1 (PD-1) blockade alone. Fifty-two patients were enrolled, with dose escalation using a Rolling 6 design followed by an expansion cohort at the recommended phase II dose (RP2D). Vorinostat was administered twice daily on days 1-5 and 8-12, and pembrolizumab was given on day 1 of each 3-week cycle. One dose-limiting toxicity (DLT) of Stevens-Johnson syndrome (SJS) and one DLT of thromboembolism were observed, establishing the RP2D. The most common adverse events were hypertension, diarrhea, and cytopenias. Among non-Hodgkin lymphoma (NHL) patients, the complete and overall response rates were notable in diffuse large B-cell lymphoma (DLBCL), particularly in primary mediastinal B-cell lymphoma (PMBL). Overall, the combination was tolerable and showed promising efficacy, especially in PMBL.
https://doi.org/10.3324/haematol.2023.283002
High-Dose Methotrexate as CNS Prophylaxis in High-Risk Aggressive B-Cell Lymphoma
In a retrospective study involving 2418 patients with aggressive B-cell lymphoma and a high risk of CNS progression, researchers investigated the efficacy of high-dose methotrexate (HD-MTX) in preventing this complication. While patients treated with HD-MTX exhibited a lower risk of CNS progression, the significance was not maintained in those in complete response at the end of chemoimmunotherapy. The study suggests that the use of HD-MTX was not associated with a substantial reduction in the risk of CNS progression in high-risk patients.
https://doi.org/10.1200/JCO.23.00365
Salvage Using PolatuzumabVedotin Based Therapy in Relapsed Refractory Large B-Cell Lymphomas
In this retrospective study conducted in India, 10 adult patients with relapsed/refractory large B-cell lymphoma failing two prior lines of therapy received Polatuzumabvedotin as salvage therapy through compassionate or named-patient access programs. The most common regimen used was Polatuzumab-Bendamustine-Rituximab. The adverse event profile was manageable, with one grade-2 infusion reaction and four patients experiencing grade 3–4 hematological toxicity. After a median of 4.5 cycles, 4 patients achieved complete response, 2 had partial response, and 3 had progressive disease.
https://doi.org/10.1007/s12288-022-01619-w
Improved survival for dose-intensive chemotherapy in primary mediastinal B-cell lymphoma
In a systematic review and meta-analysis comparing dose-intensive (DI-CIT) versus standard chemoimmunotherapy (S-CIT) for primary mediastinal B-cell lymphoma (PMBCL), data on 4,068 patients were analyzed, with 2,517 receiving DI-CIT and 1,551 receiving S-CIT. Overall survival for DI-CIT patients was significantly higher at 88% compared to 80% for the S-CIT cohort, with a meta-regression showing an 8% OS benefit for the DI-CIT group.
https://doi.org/10.3324/haematol.2023.283446
Challenges in Administering Salvage Therapy and Outcomes of Relapsed/Refractory Diffuse Large B-Cell Lymphoma
This study investigated salvage therapy patterns for patients with Relapsed/Refractory Diffuse Large B-Cell Lymphoma (RR DLBCL) in a low/middle income country (LMIC) from 2016 to 2021. Among 85 patients, most had primary refractory disease, with only 26 receiving standard salvage therapy while the rest received metronomic/palliative oral therapy. Factors associated with lack of salvage therapy included lower income, lower education level, advanced disease stage at relapse, and CNS relapse. Conversely, patients with late relapse were more likely to receive salvage therapy.
https://doi.org/10.1007/s12288-023-01693-8
Polatuzumabvedotin, venetoclax, and an anti-CD20 monoclonal antibody in relapsed/refractory B-cell non-Hodgkin lymphoma
The Phase 2 portion of this study assessed the safety and effectiveness of polatuzumabvedotin 1.8 mg/kg with venetoclax 800 mg, alongside obinutuzumab 1000 mg or rituximab 375 mg/m2, in patients with relapsed/refractory follicular lymphoma (FL) or diffuse large B-cell lymphoma (DLBCL). Key findings included a complete response (CR) rate of 59.2% in FL and 31.3% in DLBCL at the end of induction (EOI). The most common non-hematologic adverse events were manageable, with diarrhea and nausea being prevalent. Median progression-free survival was 22.8 months in FL and 4.6 months in DLBCL, suggesting promising outcomes in FL, particularly among high-risk patients.
https://doi.org/10.1002/ajh.27341
Combination Targeted Therapy in Relapsed Diffuse Large B-Cell Lymphoma
In a phase 1b–2 study, the ViPOR regimen (venetoclax, ibrutinib, prednisone, obinutuzumab, and lenalidomide) was evaluated in relapsed or refractory diffuse large B-cell lymphoma (DLBCL). Phase 1b identified venetoclax at 800 mg as the recommended dose, with manageable toxicities including grade 3 or 4 neutropenia (24%), thrombocytopenia (23%), anemia (7%), and febrile neutropenia (1%). In phase 2, among 48 evaluable DLBCL patients, objective responses occurred in 54% with complete responses exclusively seen in non-germinal center B-cell DLBCL and high-grade B-cell lymphoma with MYC and BCL2/BCL6 rearrangements. Two-year progression-free survival and overall survival rates were 34% and 36%, respectively, suggesting promising efficacy in specific molecular subtypes of DLBCL.
https://doi.org/10.1056/NEJMoa2401532
Prognostic model for relapsed/refractory transplant-ineligible diffuse large B-cell lymphoma utilizing the lymphocyte-to-monocyte ratio
In a multi-institutional retrospective study of 100 transplant-ineligible (TI) patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) following first-line R-CHOP therapy, the median age at relapse was 76 years. Progression-free survival (PFS) was 11.5 months, and overall survival (OS) was 21.9 months. Multivariate analysis identified low lymphocyte-to-monocyte ratio (LMR), elevated lactate dehydrogenase (LDH), and elevated C-reactive protein (CRP) at progression as independent predictors of OS. A predictive model, termed the Kyoto Prognostic Index for r/r DLBCL (KPI-R), based on these factors successfully stratified OS and PFS.
https://doi.org/10.1007/s12185-024-03750-y
BeEAM vs. BEAM: evaluating conditioning regimens for autologous stem cell transplantation in patients with relapsed or refractory DLBCL
This retrospective study compared BeEAM and BEAM conditioning regimens for autologous stem cell transplantation (ASCT) in 60 patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL). The study found no significant differences between the two groups in terms of time to hematopoietic reconstitution, treatment-related adverse events, hospitalization duration, or survival benefits. However, the BeEAM group had a lower hospitalization cost. The 5-year overall and progression-free survival rates were similar between the groups. The results suggest that BeEAM is a safe and cost-effective alternative to BEAM for ASCT in DLBCL patients.
https://doi.org/10.1007/s00277-024-05813-w
Primary gastric diffuse large B-cell lymphoma: A multicentre retrospective study
This study analyzed a cohort of 37 patients with stage I primary gastric diffuse large B-cell lymphoma (PG-DLBCL) from Australia, Canada, and Denmark, diagnosed between 2006 and 2018. All patients received chemoimmunotherapy, with 91.9% receiving rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP). Additionally, 35.1% underwent consolidative radiotherapy, and 18 patients were H. pylori positive, with 11 receiving eradication therapy. The 4-year progression-free survival and overall survival with R-CHOP were 88% and 91%, respectively. Interim positron emission tomography (iPET) showed promising results, and R-CHOP with iPET monitoring provided favorable outcomes, with radiotherapy and H. pylori eradication used selectively.
https://doi.org/10.1111/bjh.19470
Clinical implications of CSF-ctDNA positivity in newly diagnosed diffuse large B cell lymphoma
This study explored the clinical implications of cerebrospinal fluid (CSF) circulating tumor DNA (ctDNA) positivity in newly diagnosed diffuse large B cell lymphoma (ND-DLBCL). Among 100 patients in the training cohort, 25% had CSF-ctDNA positivity (CSF(+)), and a similar rate of 26.9% was found in the validation cohort, both significantly higher than conventional CNS involvement detection rates. Mutations in genes like CARD11, JAK2, ID3, and PLCG2 were associated with CSF(+), while FAT4 mutations showed a negative correlation. CSF(+) was linked to poorer outcomes, and a predictive model using high CSF protein, elevated plasma ctDNA, and high-risk site involvement had high sensitivity for CNS relapse prediction.
https://doi.org/10.1038/s41375-024-02279-7
Autologous stem cell transplant in fit patients with refractory or early relapsed diffuse large B-cell lymphoma that responded to salvage chemotherapy
This study retrospectively analyzed 230 patients with refractory or early relapsed diffuse large B-cell lymphoma (DLBCL) who underwent salvage therapy (ST) and autologous stem cell transplant (ASCT). Median progression-free survival (PFS) and overall survival (OS) were 16.1 and 43.3 months, respectively. Patients relapsing between 6 to 12 months after frontline therapy had better outcomes, with median PFS of 29.6 months and OS of 88.5 months. Those needing only one line of ST had significantly better survival, particularly those achieving complete response (PFS 71.1 months; OS 110.3 months). These findings suggest that ASCT remains beneficial in select chemosensitive DLBCL patients.
https://doi.org/10.3324/haematol.2023.284704
Epcoritamab in relapsed/refractory large B-cell lymphoma
Long-term results of the EPCORE® NHL-1 study with a median follow-up of 25.1 months demonstrate the sustained efficacy of epcoritamab (a CD3xCD20 bispecific antibody) monotherapy in relapsed/refractory large B-cell lymphoma (R/R LBCL). The overall response rate was 63.1%, with a complete response (CR) rate of 40.1%, and 64.2% of complete responders remained in CR at 24 months. Patients with minimal residual disease (MRD) negativity (45.4%) showed improved progression-free survival (PFS) and overall survival (OS). Epcoritamab achieved durable responses even in high-risk subgroups, with manageable safety, making it a promising option for R/R LBCL.
https://doi.org/10.1038/s41375-024-02410-8
AKT inhibitor capivasertib and the BCL-2 inhibitor venetoclax in diffuse large B cell lymphoma
The PI3K/AKT/PTEN pathway remains a promising target in B-cell malignancies, though PI3K inhibitors have limited success in relapsed/refractory diffuse large B-cell lymphoma (DLBCL) due to toxicity. Preclinical studies show that combining the AKT inhibitor capivasertib with the BCL-2 inhibitor venetoclax offers significant therapeutic benefit in DLBCL models, including those with PTEN mutations or low PTEN expression. The combination induced enhanced apoptosis and tumor growth inhibition, with the addition of rituximab further improving durability in refractory models. These findings support exploring capivasertib, venetoclax, and rituximab combinations in DLBCL treatment.
https://doi.org/10.1038/s41375-024-02401-9
Omission of Radiotherapy in Primary Mediastinal B-Cell Lymphoma
The IELSG37 trial assessed consolidation radiotherapy in PMBCL patients with complete metabolic response (CMR) after immunochemotherapy. Among 268 randomized patients, 30-month progression-free survival (PFS) was 96.2% with observation and 98.5% with radiotherapy, and 5-year overall survival was 99% in both groups. Patients with Deauville score 5 showed poorer outcomes, while omitting radiotherapy in CMR patients showed no survival disadvantage. The study supports avoiding radiotherapy in select CMR patients.
https://doi.org/10.1200/JCO-24-013
Efficacy of intravenous high-dose methotrexate in preventing relapse to the central nervous system in R-CHOP(-like)-treated, high-risk, diffuse large B-cell lymphoma patients
This systematic review and meta-analysis evaluated the efficacy of high-dose methotrexate (HD-MTX) prophylaxis in preventing CNS relapse and improving survival in high-risk diffuse large B-cell lymphoma (DLBCL) patients treated with R-CHOP or similar regimens. Based on seven observational studies (1,661 patients), HD-MTX showed a non-significant reduction in CNS relapse risk (relative risk [RR] 0.54, 95% CI: 0.27–1.07) and no survival benefit (RR 0.70, 95% CI: 0.44–1.11). The evidence quality was rated low, and the risk of bias was serious. Thus, HD-MTX appears to have limited impact in preventing CNS relapse or improving outcomes in high-risk DLBCL.
https://doi.org/10.3324/haematol.2023.284281
Analysis of CCND3 mutations in diffuse large B-cell lymphoma
Diffuse large B-cell lymphoma (DLBCL) accounts for 30–40% of newly diagnosed lymphomas, with a cure rate of approximately 60%. A study evaluating CCND3 mutations in 2059 patient samples found these mutations in 5.5% of cases, predominantly in exon 5, with hotspots including P284, R271, I290, and Q276. CCND3 mutations were associated with decreased overall survival, particularly in EZB subtype DLBCL, where they correlated with upregulated cell cycle and DNA replication pathways. These findings highlight CCND3 mutations as a novel prognostic factor, suggesting the potential for personalized therapeutic approaches to improve outcomes in affected patients.
https://doi.org/10.1007/s00277-024-05844-3
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.