
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
Cryoglobulinemia
Updated on: 19.06.25
Introduction
- Cryoglobulins are the circulating immunoglobulins that precipitate spontaneously and reversibly in serum at less than body temperature within 3 days.
- They are insoluble at 4 degree C.
- Can fix complement and initiate inflammatory reaction.
Etiology:
- Hematologic disorders
- Waldenström’s macroglobulinemia
- Multiple myeloma
- Non-Hodgkin’s lymphoma
- Chronic lymphocytic leukemia
- Monoclonal gammopathy of clinical significance
- Systemic autoimmune diseases
- Sjögren’s syndrome
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Chronic viral infections
- Hepatitis C
- Hepatitis B
- Human immunodeficiency virus
- Others (very rare): Adenovirus, herpes viruses, Epstein–Barr virus, varicella–zoster virus, human T-cell leukemia virus type 1, influenza virus, parvovirus B19, rubella virus)
- Bacterial infections (e.g., brucella, infective endocarditis, Lyme disease, rickettsia, syphilis)
- Fungal infections (e.g., coccidioidomycosis)
- Parasitic infections (e.g., echinococcosis, leishmaniasis, malaria, schistosomiasis, toxoplasmosis, trypanosomiasis)
3 types of Cryoglobulinemia- Based on immunoglobulin composition of precipitate (Both Type 2 and type 3 are called mixed cryoglobulinemia)
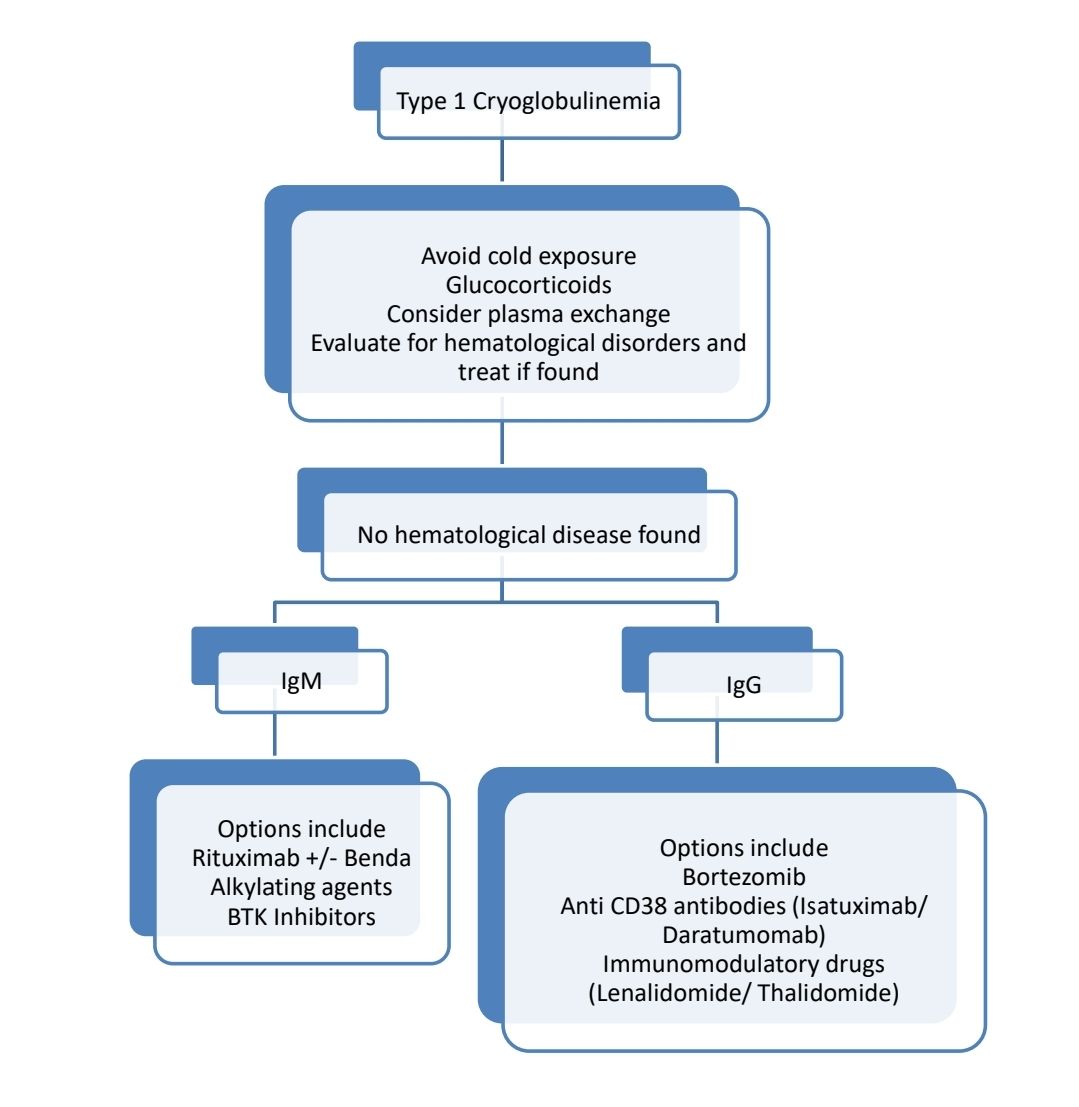
- Type 1-
- Monoclonal immunoglobins especially IgM but can be IgG or IgA
- Associated with monoclonal gammopathies of clinical significance, Waldenström’s disease, non-Hodgkin’s lymphoma, multiple myeloma, or chronic lymphocytic leukemia
- Type 2
- Monoclonal IgM mixed with polyclonal IgG
- Associated with chronic hepatitis C, autoimmune disorders
- C4 levels are low
- Type 3
- Polyclonal IgG or Polyclonal IgM or both
- Associated with lymphoproliferative disorders and connective tissue diseases
- Essential cryoglobulinemia: Do not have any underlying cause
Clinical effects:
- Type 1 Cryoglobulinemia:
- Multiple thromboses of small and medium-sized vessels (Sometimes may have signs of vascular inflammation)
- Cutaneous involvement in the form of Raynaud phenomenon, digital ischemia, livedo reticularis, and skin necrosis is common
- Joint involvement is rare
- Hyperviscosity symptoms are common
- Renal involvement is due to underlying hematological malignancy
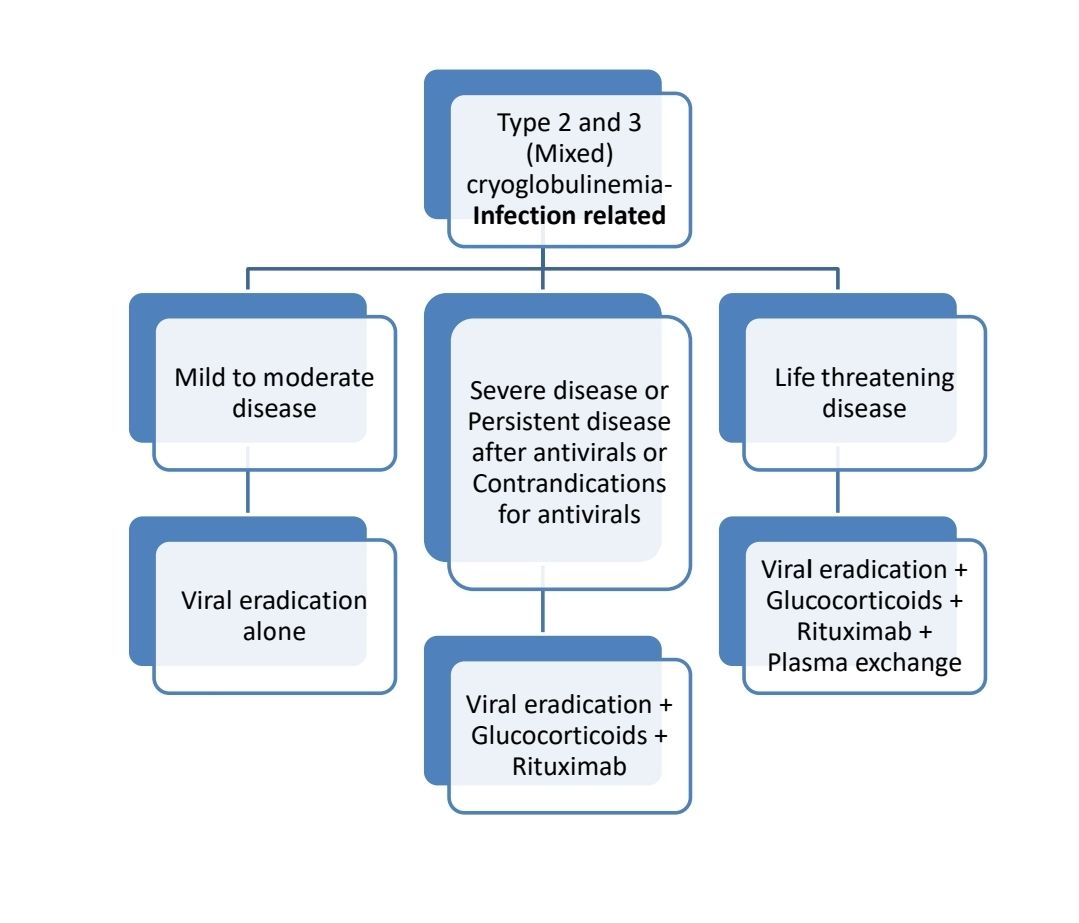
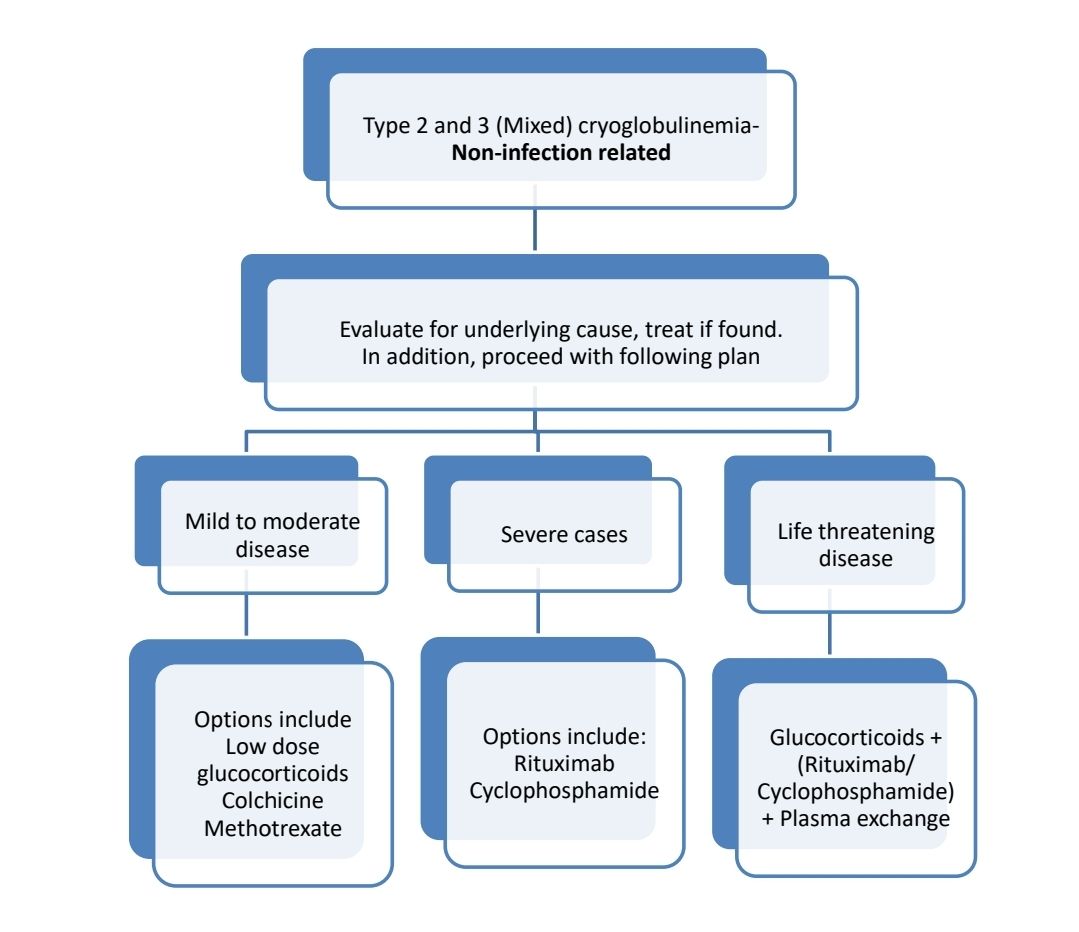
- Type 2 and 3 (Mixed cryoglobulinemia):
- Complement mediated immune-complex deposition leading to small vessel vasculitis
- Skin involvement in the form of vascular purpura is often present
- Joint and muscle involvement is present resembling Rheumatoid arthritis (But anti ccp antibody is negative)
- Neurological involvement: Sensory–motor polyneuropathy
- 1/3rd patients have renal involvement: Membranoproliferative glomerulonephritis, however end stage renal failure is rare.
Characteristic | Type I Cryoglobulinemia | Type II Cryoglobulinemia | Type III Cryoglobulinemia |
|---|---|---|---|
Range of cryoglobulin levels in serum — g/liter | 1-30 | 0.5-2 | 0.05-0.5 |
| Findings on serum protein electrophoresis | Monoclonal spike | Monoclonal spike and polyclonal elevation of gammaglobulins | Polyclonal elevation of gammaglobulins |
| Serum protein immunofixation | IgG (most often), IgM, IgA (least frequent) | Typically IgM kappa | None |
| Rheumatoid factor activity | Very rare | Frequent | Variable |
| Low C4 level | Very rare | Frequent | Variable |
| Skin biopsy | Noninflammatory thrombotic lesions with downstream infarction or hemorrhage | Leukocytoclastic vasculitis | Leukocytoclastic vasculitis, hyaline thrombi |
| Peripheral-nerve biopsy | Pauci inflammatory occlusive lesions with neuronal ischemia | Lymphocytic infiltrate around epineurial vessels, with axonal degeneration of affected nerves (vasa vasorum). Necrotising vasculitis or demyelination may be present | Lymphocytic infiltrate around epineurial vessel, with axonal degeneration of affected nerves (vasa vasorum) Necrotising vasculitis or demyelination may be present |
| Kidney biopsy | Thrombotic and hypocellular glomerular lesions | Type I membranoproliferative glomerulonephritis, endocapillary proliferation, deposits of subendothelial or intraluminal immune complexes (or both) Mesangial proliferative glomerulopathy, intraglomerular hyaline thrombi, and vasculitis with fibrinoid necrosis might be found | Type I membranoproliferative glomerulonephritis, endocapillary proliferation, deposits of subendothelial or intraluminal immune complexes (or both) Mesangial proliferative glomerulopathy, intraglomerular hyaline thrombi, and vasculitis with fibrinoid necrosis might be found |
| Direct immunofluorescence | Monoclonal immunoglobulin, usually without complement deposition | Deposits of IgM, IgG, or C3 (or combination of the three) | Deposits of IgM, IgG, or C3 (or combination of the three) |
Pathogenesis
Chronic inflammation (HCV, Autoimmune disease etc)
↓
Polyclonal lymphoproliferation and polyclonal hypergammaglobulinemia
Later, addition of monoclonal component due to autonomous lymphoproliferation (clonal expansion)
↓
Abnormal protein precipitates at low temperature in superficial veins in skin and acral parts of the body
↓
Immune complex formation with IgG and complement fractions
↓
Tissue damage in vasculature, nerves, joints and skin with monocyte-/ macrophage-infiltration
↓
Glomerulonephritis, arthralgia, purpura with haemorrhagic necrosis
Clinical features: (Meltzer’s triad: Skin purpura- often on the legs, arthralgia, and weakness)
- Skin involvement
- Infiltrated purpura: Usually gravity dependent (hence starts in lower limbs and then involves upper limbs)
- Livedo reticularis
- Nodules
- Bullae
- Cold urticaria
- Skin necrosis
- Raynaud's syndrome subsequently leading to gangrene
- Renal involvement:
- Proteinuria (nephrotic range)
- Microscopic hematuria
- Arterial hypertension
- Tubular dysfunction
- Renal failure
- Hyperviscosity in Type 1 ( if IgM is >4gm/dL):
- Blurred vision
- Vision loss, diplopia
- Deafness
- Mucosal bleeding
- Headache
- Confusion
- Vertigo, nystagmus, ataxia
- Stroke
- Joint involvement: Inflammatory, bilateral, symmetric, and nondestructive arthralgias affecting large joints
- Tenosynovitis and myalgia
- Perpheral nerve involvement:
- Sensory polyneuropathy
- Sensory–motor polyneuropathy
- Mononeuritis multiplex
- CNS involvement (Rare): Focal deficits or neurocognitive disorder
Investigations:
- Testing for cryoglobulins
- Blood sample must be kept at 37 degree C until centrifugation in laboratory
- After centrifugation of blood at 37°C, serum is stored at 4°C for 7 days and then centrifuged at 4°C
- When plasma has been frozen and then slowly thawed, cryoprecipitate appears as visible layer or band at the bottom or side of the test tube
- Further, this can be quantified
- This test is false positive in case of presence of cryofibrinogen
- LFT: Hypergammaglobulinemia
- Immunofixation electrophoresis: To identifies the constituent immunoglobulin
- C3 and C4 levels: Decreased
- Due to interference with auto-analysers: pseudoleukocytosis and pseudomacrocytosis
- Additional tests to identify underlying cause
- Biopsy of targeted tissue: May provide conclusive evidence
- Kidney: Type I membranoproliferative glomerulonephritis, with immunoglobulin and complement (C3 and C1q) deposition, endocapillary proliferation, vasculitis, or small intrarenal artery thrombosis
- Nerve: Perivascular lymphocytic infiltrate adjacent to affected nerves
- Skin: Vasculitis or small vessel thrombosis
Prognosis:
- HCV associated mixed cryoglobulinemia
- 25 to 30%- Remain asymptomatic
- 40 to 45%- Mild cutaneous manifestations
- 20 to 30%- Significant organ damage
- 7 to 12%- Progress to B-cell lymphoma
- 2 to 5%- Rapidly progressive and life-threatening vasculitis
- Type I cryoglobulinemia: 5-year overall survival is 77 to 83%
Poor prognostic markers:
- Non–HCV-related cryoglobulinemic vasculitis (including HBV related disease, underlying autoimmune diseases, and essential forms)
- Male patients with purpura
- Type II cryoglobulinemia
Treatment Plan:
Autoimmune disease related cryoglobulinemia: Low-dose interleukin-2 may be used. It may be used in other types of cryoglobulinemia which are refractory to above treatments.
Defining features for severe disease:
- Glomerulonephritis with impaired renal function
- Motor deficit
- Multiple mononeuropathy
- Digital ischemia/ Extensive skin necrosis
- Digestive, cardiac, or pulmonary involvement
Relapsed disease:
- Retreatment with Rituximab again
About each modality of treatment:
- Rituximab:
- 375 mg per square meter of body-surface area
- On days 1, 8, 15, and 22
- In severe or life threatening cases, may consider maintenance Rituximab
- May cause drug-induced vasculitis flare, similar to serum sickness (between days 2 and 9 after rituximab infusion, with associated mortality exceeding 50%.)
- Use with caution in patients with HBV associated cryoglobulinemia. Adequate prophylactic therapy for HBV infection, or monitoring HBV DNA or HBsAg title should be done
- Steroids:
- 0.5–1.0 g of methylprednisolone for 3 consecutive days, followed by tapering doses of oral prednisolone
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.