
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
EBV Postive T-NK lymphomas (Includes Extranodal NK-T cell lymphoma)
This category includes following disorders:
- Extranodal NK/T-cell lymphoma
- EBV-positive nodal T- and NK-cell lymphoma
Extranodal NK/T-cell lymphoma
Introduction:
- Presents as lethal midline granuloma of nose.
Epidemiology:
- Common in Asians and native Americans
- Increased association with haplotypes: HLA-DPB1, HLA-DRB1 and IL18RAP
Etiology:
- Most are associated with EBV infection
- Immunosuppressed state
Clinical Features:
- Facial edema
- Nasal obstruction/ epistaxis
- Midfacial destruction with extension into orbits, sinuses and oral cavity
- Systemic symptoms- Fever, malaise, weight loss
- Some cases- Hemophagocytic syndrome
- Regional lymph nodes may be involved
Investigations:
- Tissue biopsy
- Biopsy has to be taken from the edge of the lesion and from apparently uninvolved site, as there is often extensive necrosis.
- Mucosal sites show extensive ulceration
- Diffuse lymphomatous infiltrate
- Angiocentric&angiodestructive growth pattern is usually present
- Fibrinoid changes may be seen in vessel walls
- Coagulative necrosis and apoptotic bodies are very common
- Tumor cells show wide spectrum of morphology– small / medium / large / anaplastic
- Tumor cells have irregular or elongated nuclei with granular chromatin and iinconspicuous nucleoli. Cytoplasm is moderate and pale to clear .
- They may show heavy admixture of inflammatory cells including small lymphocytes, plasma cells, histiocytes and eosinophils (so also called as polymorphic reticulosis)
- Immunophenotyping by immunohistochemistry
- Positive – CD56, CD2, Cytoplasmic CD3ε, Cytotoxic granule associated protein CD43, CD45RO, HLA-DR, IL2 receptor, fas&fasligand
- Negative – Surface CD3 and other T & NK cell associated antigens (CD4, CD5, CD8, TCRb, TCRd, CD16, CD57)
- In situ hybridization for EBER- Positive
- Molecular studies
- T Cell receptor & immunoglobulin genes are in germ line configuration
- EBV can be demonstrated (Clonal episomal form)
- Mutation of TP53, beta catenin, K-RAS, c-KIT
- Cytogenetics
- del (6) (q21 q25)
- i(6) (p10)
- Gain of 2q and loss of 1p, 6p and 4q
- MRI- To note the extension of disease
- PET-CT
- To identify occult disease
- This is must, as, if tumor is localized it is curable by radiotherapy
- EBV PCR (Viral load)-
- Helpful in monitoring of disease
- May have prognostic relavance
Prognosis:
- Poor
- With disseminated disease overall survival is few months
- With sequential chemo-radiotherapy 5 year survival- >70% with early stage disease
- Prognostic index of Natural Killer Lymphoma: Risk factors include
- Age >60 years
- Stage III or IV disease
- Distant lymph node involvement
- Non-nasal type disease
Number of factors | Risk Category |
0 | Low |
1 | Intermediate |
>1 | High |
- Other unfavorable prognostic markers:
- B Symptoms
- Elevated LDH
- Bone/ skin involvement
- Expression of p19
- Ki67- >50%
- Raised CRP level
- Anemia
- Thrombocytopenia
- High serum EBV levels
- EBV positive cells in bone marrow
Pretreatment Work-up:
- History
- B-Symptoms
- Examination
- LN:
- Spleen:
- ENT- Includingnasopharynx:
- Complete Skin exam:
- Testicles
- WHO P. S.
- BSA
- IHC
- BMA and Bx
- CT (CAP)/ PET
- MRI+/-CT Nose/PNS/Palate
- Stage
- Hemoglobin
- TLC, DLC
- Platelet count
- LFT: Bili- T/D SGPT: SGOT: Albumin: Globulin:
- Creatinine
- Electrolytes: Na: K: Ca: Mg: PO4:
- Uric acid:
- LDH
- HIV:
- HBsAg:
- HCV:
- EBV Viral load
- UPT
- PINK score
- ECHO (If anthracyclines planned)- LVEF- %
- RT Consulation for Pre-Rx Evaluation
- Chemotherapy consent after informing about disease, prognosis, cost of therapy, side effects, hygiene, food and contraception
- Fertility preservation
- PICC line insertion and Chest X ray after line insertion
- Tumor board meeting and decision
- Attach supportive care drug sheet
- Inform primary care physician
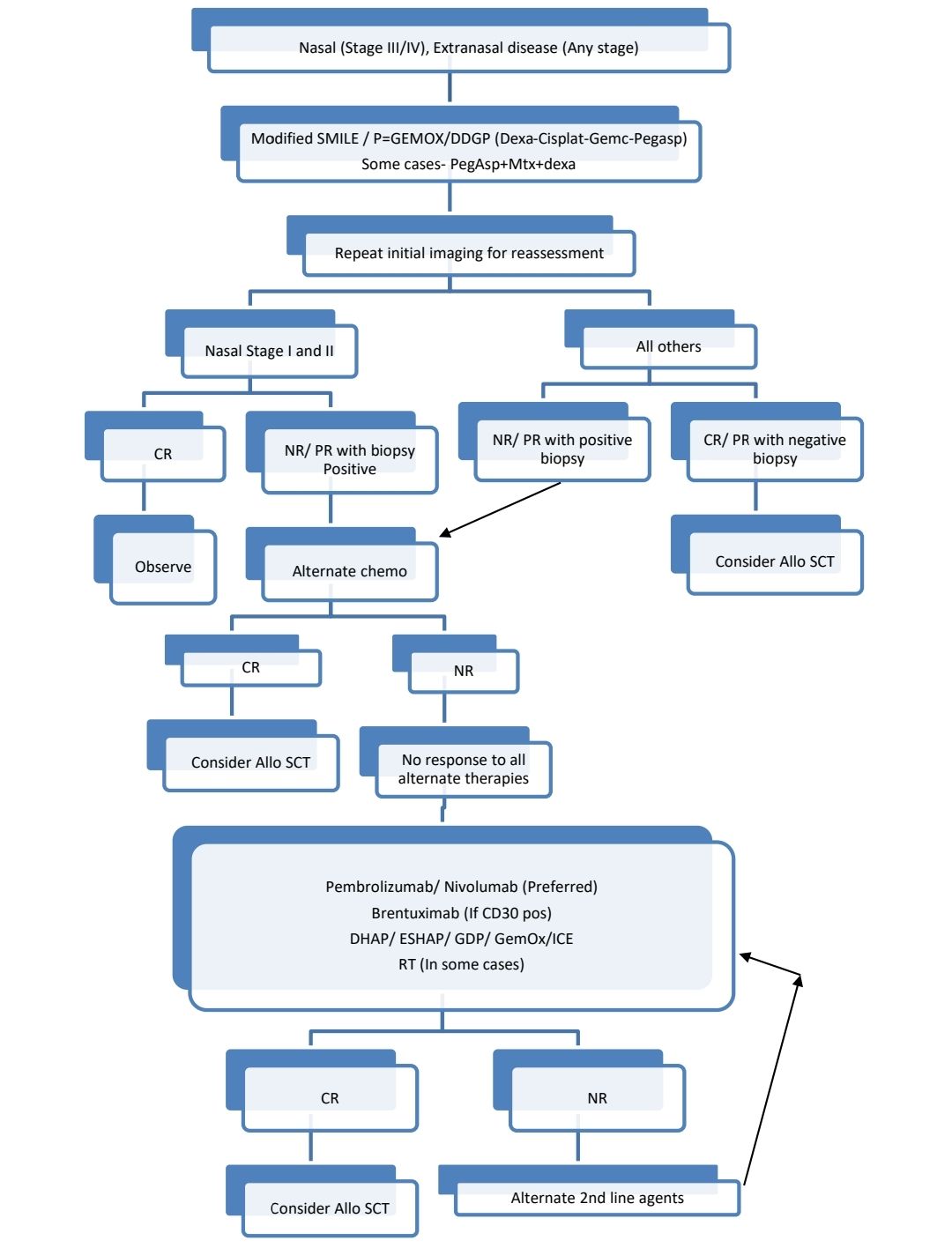
Treatment Plan:
- Nasal
- Limited disease (Stage 1 and 2)
- If fit for chemotherapy treat like advanced stage of disease
- If not fit for chemotherapy- RT and observe
- Limited disease (Stage 1 and 2)
Radiotherapy:
- Involved field radiotherapy
- 50Gy
Related Disorders:
- Extranasal NK T cell lymphoma
- Involves skin, testes, GIT
- Careful ENT evaluation is must, to rule out occult primary
- Tumor cells are EBV positive
EBV-positive nodal T- and NK-cell lymphoma
- It is an EBV-positive lymphoma of cytotoxic T- or NK-cell lineage, presenting primarily with nodal disease
- Presents with lymphadenopathy, B symptoms and thrombocytopenia
- Rare
- Median age: 60-64 years
- Micro: Architectural effacement by a diffuse infiltrate of medium to large lymphoid cells (centroblastic)
- IHC:
- Positive: pan T-cell markers (such as CD3 and CD2), cytotoxic molecules (TIA1, granzyme B, and perforin), CD8 and CD56
- Negative: CD4 and CD5
- EBER- Postive in most of tumor cells
- Median survival: 2-8 months
Recent advances:
Efficacy of a short sandwich protocol, methotrexate, gemcitabine, L-asparaginase and dexamethasone chemotherapy combined with radiotherapy, in localised newly diagnosed NK/T-cell lymphoma
A retrospective multi-centre study evaluated the efficacy of the MGAD regimen combined with radiotherapy in 35 patients with localized extranodal NK/T-cell lymphoma. 91% of patients achieved complete remission, with progression-free and overall survival rates at 2 and 5 years of 71%, 80%, and 53%, 73%, respectively. About one third of patients experienced relapse within 14.5 months. Manageable side-effects included cytopenias, mucositis, and infection. Asparaginase activity monitoring showed drug inactivation in 54% of patients. These findings suggest that the sandwich MGAD chemoradiotherapy is a tolerable and effective treatment option for localized extranodal NK/T-cell lymphoma.
https://doi.org/10.1111/bjh.18689
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.