
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
Infectious Diseases Related to Hematology Practice
Predisposing factors for infections in hematology patients:
- Impaired cell mediated immunity(Ex: Fludarabine)- Increased risk of PCP, VZV, CMV etc
- Impaired humoral response (Ex: Rituximab)- Increased risk of HBV reactivation
- Steroids- Negative effect on glucose homeostasis, wound healing, skin fragility, monocyte and lymphocyte function, production of cytokine and humoral immune responses
- Broken mucosal barrier due to chemotherapy, leading to infection by commensals
- Immunosuppression following HSCT
- Neutropenia- Due to leukemia, aplastic anemia or chemotherapy
- Defective function of neutrophils in case of MDS.
- Decreased protective immunoglobulins and defective complement as in multiple myeloma.
Vaccinations which can be done in patients treated for blood cancer:
- For all:
- Annual influenza vaccine (Inactivated)- Start 6 months after last chemotherapy
- Pneumococcal vaccine(PCV 13)- 3 doses 1 month apart. Start 6 months after last chemotherapy
- dTP- 3 doses- 0, 1month and 6 months- Start 6 months after last chemotherapy.
- HPV- In previously unvaccinated females and males between 11-26years- 3 doses- start 6 months after last chemotherapy
- Special circumstances and for HSCT patients:
- Hepatitis B- 3 doses- Start 6 months after last chemotherapy
- H. Influenza type B- 3 doses. Start 6 months after last chemotherapy
- Meningococcal conjugate vaccine(MCV-4)- Single dose- To be given only is there is an outbreak situation.
- Typhoid bacterial capsular polysaccharide
- Inactivated polio vaccine- 3 doses- 6 months after last chemotherapy
- Avoid live vaccinations (MMR) in HSCT survivors with active GVHD or on-going immunosuppression- It can be given later on
- Do not give- Live influenza vaccine, Live zoster vaccine, oral polio, rota virus, oral typhoid and yellow fever vaccines.
Herpes Simplex
Mode of infection:
- Exposure to mucosal surface, abraded skin
Incubation period: 1-26 days (Median- 6-8 days)
Pathogenesis:
Entry of virus through the defects in the skin and mucus membrane
↓
Replication of virus in cells of epidemis and dermis
↓
Infection of either sensory/ autonomic nerve endings
↓
Entry into neuronal cells
↓
Transported intra-axonally to the nerve cell body in ganglia
↓
Replication of virus in ganglia and contageous neural tissue
↓
Virus remains latent in trigeminal nerve (HSV-1), Sacral nerve (HSV2)
↓
Reactivation upon exposure to sun/ mental stress/ fever/ immunosuppression of any cause/ menstruation
↓
Herpes labialis (Thin walled umbilicatedvesicles, which later form superficial ulcers)
↓
Genital lesions- Urethritis, cervicitis, vaginitis, vulvitis
Investigations:
- Tzanck smear- Scrapings from the base of lesion
Complications:
- Encephalitis
- Meningitis
- Visceral infection- Esophagitis, pneumonitis, hepatitis
- Adrenal necrosis
- Bell's palsy
- Keratitis
- Fetal infection
Treatment:
- Acyclovir
- If resistant: Foscarnet/ Cidofovir
Varicella Zoster
Mode of infection:
- Droplet infection
Pathogenesis:
Infection through respiratory route
↓
Localized replication occurs in nasopharynx
↓
Seedling of respiratory reticuloendothelial system
↓
Viremia/ Chickenpox
↓
Latent virus in dorsal route ganglia
↓
Reactivation when immunity is compromised
↓
Virus travels across the sensory nerve
↓
Herpes zoster
Clinical features:
- Severe and continuous pain along the distribution of affected nerve root (Common in T3 and L3)
- Skin rash in affected area, later forming vesicles
- Segmental muscle wasting
- Ramsay Hunt syndrome- Unilateral facial palsy with vesicles on auricle and palate
Complications:
- Neurological- Meningo-encephalitis, Granulomatousangiitis leading to contralateralhemiplegia, transverse myelitis with or without motor paralysis
- Post-herpetic neuralgia
Treatment:
- Acyclovir
- Post herpetic neuralgia- Amitriptyline/ Gabapentin
Cytomegalovirus
Mode of infection:
- Contact with infected saliva/ urine
- Sexual contact
- Transmission during child birth/ breast feeding
Pathogenesis:
Major envelop glycoprotein of CMV binds to epidermal growth factor receptor
↓
Infects and remains latent in WBC
↓
Reactivated when cellular immunity is decreased
↓
Various clinical manifestations
Clinical features:
- Primary infection: Infectious nucleosis like syndrome
- Reactivation: (Usually seen 30-100days post-transplant. It can also be seen with use of Ruxolitinib and Idelalisib)
- Fever
- Weight loss, malaise, myalgia
- Splenomegaly
- Hepatitis
- Pneumonitis
- Retinitis
- Enteritis
- Encephalitis/ transverse myelitis
- Severe forms of reactivation:
- Progressive pulmonary infiltrate
- Pancytopenia
- Pancreatitis
- Hypotension
- Indirect effects of reactivation
- Increased risk of graft failure
- Bacterial/ fungal superinfection
Investigations:
- Quantitative PCR for viral load (May be negative in GI involvement by CMV)
- Biopsy of infected tissue: Cytomegalic cells
- Found in almost all organs
- 2-4 times larger than surrounding cells
- Intranuclear inclusions- 8-10microns, eccentrically placed, surrounded by clear halo (Owl's eye appearance)
- Smaller intracytoplasmic inclusions
Prognosis:
- If untreated, high rates of mortality
- With treatment, resolution rate- 50-70% (in non ventilator dependent patients)
Prevention:
- Selection of donor (CMV IgG antibody testing must be done prior to the transplant):
- CMV negative donor must be chosen for CMV negative recipient
- CMV positive donor must be chosen for CMV positive recipient
- Provide CMV safe blood products: Leucodepleted/ blood from CMV negative donors
- Primary prophylaxis
- Valacyclovir- 2gm- QID- (Better to give prophylaxis for 90 days post transplant. Otherwise keep monitoring viral load. It is useful only for prophylaxis , not for treatment)
- Using Ganciclovir leads to higher risk of development of resistance
- Quantitative PCR for CMV DNA weekly for 3 months post transplant. In positive patients and those with GVHD monitoring should be continued for 6 months.
- Vaccines: Live attenuated (Towne 125)/ Plasmid DNA/ Purified CMV polypeptide are being tried in clinical trials.
Treatment: (Presence of CMV viremia is a strong predictor of subsequent clinical illness. Almost 60% develop pneumonitis)
- Inj. Ganciclovir- 5mg/kg in 100ml NS over 1 hr- BD
- Given usually for 14 days, then if viral load declines to <300copies/ml- OD for 2 weeks
- T. Valganciclovir is substitute for Ganciclovir. Dose- 900mg-BD-PO
- If during treatment viral load persists/ increases- consider drug resistance and to sequence analysis for UL 97 and UL 54 gene mutations.
- IV Immunoglobulins- 400mg/Kg- every 48hrs for 7-10 doses then once a week for 4 weeks (Useful especially if there pneumonitis)
- Make an attempt to decrease/ stop immunosuppression especially steroids. Switch to Sirolimus as it has anti-CMV properties
- If resistant
- Cidofovir- 5mg/kg per week for 3 weeks
- Foscarnet- 60mg/kg, IV- BD (It can be used as first line agent, if there is persistent ganciclovir induced neutropenia)
- Based on viral load (These targets vary in different centers, based on PCR methodology)
- <60 copies/ml- Valacyclovir prophylaxis
- 60-300 copies/ml- OD treatment
- >300 copies/cmm- BD treatment
Infectious Mononucleosis
Causative agent: Ebsteinbarr virus
Mode of infection:Oral contact with exchange of saliva
Incubation Period: 4-5 days
Pathogenesis:
Infection of epithelium of oropharynx through CR2 receptor
↓
Local multiplication in tonsils and invasion of blood stream
↓
Infection of susceptible B lymphocytes by attaching to their CD21/ specific c3d receptor on the cell surface
↓
Multiplication of lymphocyte and bursting of lymphocyte
↓
Further infection of B cells
↓
Polyclonal activation of B lymphocytes leading to many kinds of immunoglobulins
↓
Proliferation of CD8+ cells to control infection (leads to inversion of CD4/CD8 ratio)
↓
Control of infection
But virus remains in B cells throughout lifespan, but expresses only EB nuclear antigen 1 which does not elicit T cell response
Clinical features: (Teenagers are commonly affected)
- Prodromal symptoms- Malaise, tiredness, headache, myalgia, anorexia, abdominal discomfort, fever
- Sore throat, exudative tonsillitis
- Petechial rash on palate
- Lymphadenopathy, splenomegaly, hepatomegaly
- Maculopapular rash if Amoxycillin is given
Investigations:
- Peripheral smear- Leucopenia in initial stage followed by lymphocytosis. Atypical lymphocytes (>10%) are seen.
- Paul Bunnel test: Heterophile antibodies agglutinate sheep RBCs
- Monospot test
- EBV viral load
- Detection of IgM antibody against viral capsid antigen
- LFT- Deranged with cholestatic findings
Prognosis: Self limited in majority of patients
Complications:
- Respiratory: Severe pneumonia
- CNS: Aseptic meningitis, encephalomyelitis, transverse myelitis, GuillainBarre syndrome, chronic fatigue syndrome, cranial nerve palsies
- Hematological: Immune hemolytic anemia, thrombocytopenia, aplastic anemia, hemorrhage, hemophagocyticlymphohistiocytosis, splenic rupture
- Chronic active EBV infection: Fever, bone marrow hypoplasia, interstitial pneumonia, hepatosplenomegaly, persistent hepatitis, lymphadenitis, uveitis, hydroavacciniforme in skin, hypersensitivity to mosquito bites
- Duncan syndrome: X linked immunoproliferative disease
- Oral hairy leukoplakia
- Others: Myocarditis, pericarditis, hepatitis, glomerulonephritis, orchitis
- EBV induced neoplasms (LMP1 activated NFk beta pathway and JAK2 signaling pathway, EBNA-2 gene transactivates cyclin D and members of SRC family)
- Post transplant lymphoproliferative disorders
- African Burkitt's lymphoma
- Hodgkin lymphoma
- T and NK cell lymphoma
- Nasopharyngeal carcinoma
- Leiomyoma and leiomyosarcoma
- Gastric carcinoma
- Lymphoma in HIV patients
Treatment:
- Self limiting disease, hence give only symptomatic treatment
- Steroids if there is severe dysphagia, AIHA, ITP, Neurological complications, pancreatitis, myocarditis
- Acyclovir if there is post transplant EBV infection or chronic active EBV infection
Note: Infectious mononucleosis like syndrome can be caused by CMV, adeno virus, viral hepatitis, HIV, rubella, HHV-6, Metapneumovirus, bartonellahensale, brucellaabortus, toxoplasmagondii
Dengue
Introduction:
- Caused by favivirus with distinct serotypes- DV-1, DV-2, DV-3, and DV-4.
- Endemic to tropical countries
- Epidemics are seen following each rainy season
- Most of the patients develop simple febrile illness, while small proportion of patients develop shock syndrome.
Incubation period: 2-7 days
Mode of infection: Bite of Aedisaegiptii
Pathogenesis:
Production of antibodies against virus
↓
Activation of cross reacting CD4 and CD8 T lymphocytes
Activation of complement system
↓
Release of cytokines
↓
Plasma leakage and hemorrhage
Clinical features:
- Prodrome (2days): Malaise, headache, prostration
- Acute onset (7-8 days): Fever, headache, body ache, retrobulbar pain, arthralgia, myalgia, vomiting, relative bradycardia, inflamed throat, tender hepatomegaly, lymphadenopathy, centrifugally spreading macular rash
- Convalescence (Slow recovery)
Investigations:
- Hemogram:
- Leucopenia, thrombocytopenia, increased hematocrit
- Drop in platelet count to <1,00,000/cmm is an indicator that the patient is at risk of entering the critical phase in next 24 hrs.
- Serum antigen detection- NS1 antigen
- Serum antibody detection- IgG, IgM
Complications:
- Dengue hemorrhagic fever (Dengue shock syndrome)
- Thrombocytopenia with hemoconcentration
- Fever
- Hypotension
- Capillary leak syndrome causing extravasation of fluids
- Grading: I- Fever with positive tourniquet test, II- Spontaneous bleeding, III- Circulatory failure, IV- Profound shock
- MODS: Encephalopathy, liver failure, renal failure
- Secondary infection and sepsis
Treatment:
- Grade I:
- Symptomatic treatment- Paracetamol- For pain and fever
- Rest
- Grade II: Hydration- Oral as much as possible. IV if patient is unable to take orally.
- Grade III and IV:
- Platelet transfusion: If platelet count is less than 20,000/cmm
- PRBC transfusion, if there is internal bleeding.
- Careful fluid balance maintaining adequate filling of intravascular compartment while avoiding fluid overload later on. After critical phase is over, fluid in extravascular compartment returns to intravascular compartment, which can lead to CCF and pulmonary edema. Adequate filling of intravascular compartment can be assessed by postural drop in blood pressure and postural tachycardia.
- Treatment of circulatory failure
- Steroids/ IVIg are not found to be beneficial
Viral hemorrhagic fevers (Caused by Arbo viruses)
- Alfa viruses: Chikungunya
- Flavi viruses: Dengue, Yellow fever, Kyasnur forest disease, Omsk hemorrhagic fever
- Bunya: Crimean Congo Hemorrhagic fever
Influenza and parainfluenza:
- Diagnosis is by nasopharyngeal swabs (PCR)
- Chemoprophylaxis/ Treatment: Inhaled Zanamivir- 10mg- BD- for 5 days/ Oseltamavir- 75mg- BD for 5 days
Respiratory synciatial virus
- Treatment: AerosolizedRibavarin with IVIg
Human metapneumovirus
- No treatment is required for most of the cases
- Severe symptoms- IVIg
Human Rhinovirus
- No specific treatment is available at present
BK Virus
- Associated with encephalitis, hepatitis, cystitis
- Investigation: Urine PCR for BK virus
- Treatment
- Quinolones
- Cidofovir- Intra vesicular/ IV
Human herpes virus 6
- Reactivation is seen in 5-70% of HSCT patients
- Presents with encephalitis with characteristic limbic/ hippocampal derived symptoms
- Skin rash- predominantly on cheeks
- Investigations:
- MRI
- EEG
- CSF for HHV-6 DNA
- Treatment:Foscarnet/ Ganciclovir
Parvovirus B 19
- Causes erythemainfectiosum (5th disease)
- Mode of infection: Respiratory secretions
- Incubation period: 4-14 days
- Clinical features: 3 stages
- Slapped cheek
- Itchy maculopapular rash on trunk and extensor aspect of limbs
- Disappearance of rash from center
- Complications:
- Arthritis
- Aplastic anemia in children with chronic hemolysis
- Pure red cell aplasia
- Intra-uterine infection can lead to hydropsfetalis
- Treatment: Not required for uncomplicated infection
Invasive Aspergillosis
Causative agents:
- A. Fumigatus
- A. Flavus
- A. Niger
- A. terreus
Clinical types of aspergillosis:
- Noninvasive aspergillosis
- Allergic bronchopulmonary aspergillosis (Not discussed further)
- Allergic fungal rhinosinusitis (Not discussed further)
- Aspergilloma (Not discussed further)
- Invasive aspergillosis
- Pulmonary
- Tracheobronchial (Ulcerative lesions/ pseudomembranes)
- Sinuses
- Cerebral
- Hepatosplenic
Source of infection: Inhalation of Aspergillus conidia (eg spores) which is ubiquitously present (soil and in decaying vegetative material)
Predisposing conditions:
- Immunosuppressive therapy especially for GVHD
- Prolonged neutropenic due to chemotherapy
- Following allogenic bone marrow transplantation (first 2 weeks to 4 weeks)
- Following solid organ transplantation
- Coinfection with immunomodulatory viruses such as cytomegalovirus
- Respiratory viral infections: avian influenza H7N9, influenza A, influenza B, respiratory syncytial virus, SARS-CoV-2 etc
- Comorbidities: Type 2 DM, CKD
- COPD with accompanying corticosteroid use
- Drugs: Ibrutinib
Clinical features:
- Pulmonary: Fever, cough, chest or pleuritic pain, shortness of breath, hemoptysis
- Sinus: Pain over the sinuses, swelling, epistaxis, nasal obstruction, cacosmia, cranial nerve involvement, orbital involvement
- Ocular: keratitis, periorbital cellulitis with or without the orbital apex syndrome, endophthalmitis, vitritis
- Osteomyelitis: Rare, seen in trauma patients
- CNS: Brain lesions, meningitis
Investigations:
- CT scan:
- Initially infiltrates, consolidation, or mass-like lesions with or without pleural effusions
- Halo sign: Area of low attenuation surrounding a pulmonary nodule
- Air crescent sign: Develops during neutrophil count recovery
- Bronchoscopy or other scopies for visualization of lesion and getting sample for KOH preparation, Galactomannan, biopsy, Fungal culture, molecular methods for differentiation
- Microscopy:
- Thin branching hyaline hyphae
- Angioinvasion
- Culture on fungal specific media
- Serum galactomannan antigen:
- Sensitivity- 50%
- False positive results with some foods and with piperacillin with tazobactum
- Useful as prognostic marker as well, as declining trends over 7 to 14 days indicate response to therapy
- Other Aspergillus spp antigen detected in serum is Aspergillus beta D glucan
- PCR for Aspergillus
- Nucleic acid–based assays based tests for assessing sensitivity
- Breath metabolite signatures
Prognosis:
- Mortality with invasive aspergillosis is very high
Prophylaxis:
- Posaconazole: Tablet/IV: 300 mg BD on day 1, then 300 mg daily
- Voriconazole: Dosing same as for treatment
- Itraconazole suspension: 200 mg PO every 12 h
- Micafungin: 50 mg/d
Treatment:
- Antifungals
- Voriconazole: Treatment of choice
- 6 mg/kg IV, every 12 hours for 2 doses, followed by 4 mg/kg every 12 hours
- PO. 200 mg twice a day
- Amphotericin: 1mg/kg- IV- OD
- Liposomal amphotericin- 3– 5 mg/kg/d IV
- Caspofungin- 70 mg/d, IV stat followed by50 mg IV- OD
- Micafungin: 100– 150 mg/d IV
- Posaconazole:
- Syrup: 5ml- TID PO with ghee
- Tablet: 300mg BD on day 1, then 300mg daily
- IV: 300 mg BD on day 1, then 300 mg daily
- Itraconazole:
- Used primarily in noninvasive or chronic forms of aspergillosis
- 200mg PO every 12 h
- Isavuconazole: 200-mg PO, 3 TID for 6 doses, followed by 200 mg OD thereafter
- Voriconazole: Treatment of choice
- Indications for combination antifungals (Usually voriconazole with caspofungin)
- Severe sepsis
- Respiratory failure
- CNS involvement
- Invasive aspergillosis of sinuses:
- Surgical debridement and debulking of the site
- Reduction of immunosuppression
- Antifungal therapy
- Tracheobronchial aspergillosis
- Along with systemic antifungal inhaled AmB may be useful
Different types of treatment
- Prophylactic: Antifungals given to prevent infection
- Emperical: Fever is present, but none of the tests are positive. Patient continues to have fever spikes in spite of good coverage by antibiotics.
- Pre-emptive: Treatment based on positive serological tests or CT scan report
- Definitive: Treatment after culture or histopathology is positive for fungus
Mucormycosis
Causative agents:
- Rhizopus spp
- Mucor spp
- Lichtheimia spp
- Rhizomucor spp
- Cunninghamella spp
- Apophysomyces spp
- Saksenaea spp
Source of infection
- Decaying vegetations
Route of infection
- Inhalation of sporangiospores
Predisposing factors:
- For sinus and lung infection: Poorly controlled diabetes mellitus, organ/ hematopoietic stem cell transplantation patients, hematological malignancy, long term desferoxamine therapy
- For GI infection: Uremia, severe malnutrition, diarrheal diseases
Clinical features:
- Sinus infection: Low grade fever, unilateral facial edema, dull sinus pain, nasal congestion, thin bloody nasal discharge, diplopia due to decreased extra-ocular muscle movements, chemosis, proptosis, blindness due to globe/ ophthalmic artery invasion, coma due to invasion of frontal lobe
- Lung: Progressive severe pneumonia, high grade fever, spread of infection through the diaphragm into the abdomen
- Gastrointestinal: One or more ulcers which tend to perforate
- Renal mucormycosis
- Cutaneous and soft-tissue mucormycosis (usually secondary to trauma): Abscesses, skin swelling, necrosis, dry ulcers, and eschars
Investigations:
- CT and MRI-
- Sinus: Opacification of one or more sinuses, associated with local extension
- Chest: Reverse Halo sign (an area of ground glass opacity surrounded by a ring of consolidation), >10 nodules, pleural effusion, vessel occlusion on CT pulmonary angiography
- Renal: enlarged, non-hydronephrotic kidneys with hypodensities, cortical rim sign
- Abdominal: isolated abdominal mass
- CT sinuses, chest, abdomen, pelvis- For staging purposes
- Carotid arteriography: Invasion/ obstruction of carotid siphon
- Biopsy (Endoscopic, or CT-guided): For KOH preparation and histopathology
- Direct microscopy using flourescent brightener and histopathology with special stains (eg PAS and GMS)
- Non-septate/ pauci-septate, ribbon-like hyphae (at least 6–16 μm wide)
- 90° branching angle
- Haemorrhagic infarction, coagulation necrosis, angioinvasion, infiltration by neutrophils (in non-neutropenic hosts), and perineural invasion
- Splendore-Hoeppli phenomenon: Hyphae covered by the deeply eosinophilic material
- Culture on routine media at 30°C and 37°C
- Strongly recommended for genus and species identification and for antifungal susceptibility testing
- Cottony white or grayish black colony
- Molecular identification preferably semi-nested qPCR, HRM, Multiplex Target: 18s, ITS, 28s or rDNA
- Immunohistochemical staining with specific primary reagents
- Susceptibility testing
Prognosis:
- All-cause mortality rates: 40% to 80%
- Poorest prognosis in patients with haematological malignancies and HSCT recipients
- CNS involvement is associated with mortality rates higher than 80%
Treatment:
- Urgent intervention must be done whenever there is suspicion of mucormycosis. Delayed initiation of therapy is associated with increased mortality
- Control of blood sugar
- Extensive debridement +/- orbital exenteration with clean margins
- For 3 purposes: disease control, histopathology, microbiological diagnostics
- Liposomal amphotericin B-
- Routine: 5–10 mg/kg per day from day 1
- If brain involvement: 10 mg/kg per day from day 1
- If solid organ transplant patient: 10 mg/kg per day from day 1
- If preexisting renal compromise
- Isavuconazole IV: 200 mg TID for 2 days followed by 200 mg per day, if good response PO administration can be done in same dose
- Posaconazole IV: 300 mg BD on day 1, then 300 mg OD, if good response PO administration can be done in same dose
- For orbital disease: Retrobulbar injection of amphotericin B deoxycholate in addition to systemic therapy
- If there is progressive disease/ severe toxicity: Change to alternate antifungal
- Duration of therapy:
- Not clearly known
- Usually antifungals are given for weeks to months
- Antifungals must be continued until
- Permanent reversal of immunosuppression
- Resolution of signs and symptoms of infection
- Substantial radiographical improvement
- After initial treatment with Liposomal amphotericin for 3-4 weeks, switching to oral treatment, use of isavuconazole or posaconazole, may be done
Candidiasis
Causative agent:Candida albicans
Predisposing Factors:
- Prolonged neutropenia
- AIDS
- Pregnancy
- Diabetes
- Birth control pills
- Young and old age
- Trauma
- Corticosteroid therapy
- Treatment with antibiotics
Clinical features:
- Oral thrush
- Vulvovaginitis- White discharge
- GI candidiasis- Diarrhea
- Esophageal candidiasis- Retrosternal pain and dysphagia
- Cutaneous- Intertriginous skin is affected. Erythematous moist/ scaly lesion
- Paronychia
- Systemic
- Bronchopulmonary
- Hepatospleniccandidiasis
- Endocarditis
- Meningitis
- UTI
Investigations:
- Microscopy- Wet film and gram stain (Budding yeasts/ pseudohypae are seen)
- Culture on SDA medium- Creamy, white colonies with yeasty odour
Treatment:
- Local infection:
- Topical- Clotrimazole
- Tab. Fluconazole
- Systemic infection:
- Rapidly remove the catheter irrespective of the Candida species.
- Echinocandins or Liposomal amphotericin- for 6-8 weeks
- Then- Fluconazole for 1 year or till all lesions disappear
PneumocystisCarinii
Route of transmission: Airborne inhalation
Incubation period: 4-8 weeks
Predisposing factors:Immunosuppressed states- HIV patients, immunosuppressive therapy, organ transplantation, children with primary immunodeficiency disease
Pathogenesis:
Inhalation
↓
P. carinii attaches to type 1 cells in alveoli
↓
Once immunity is decreased, it multiplies and fills the alveoli
↓
Pneumonia
Treatment:
- Cotrimoxazole- 10mg/kg/day
- Pentamidine
- Dapsone
Malaria
Introduction
- Overall 350 million cases every year with 1million deaths
- Most of them occur in south east Asia
- More common in November
Causative agents: Plasmodiumfalciparum, Pl. vivax, Pl. Ovale, Pl. Malariae
Incubation period: 10-14 days
Mode of infection: Bite of infected female anopheles mosquito
Following people are immune: Sickle cell disease, Beta thalassemia, G6PD deficiency, Duffy negative blood group, south east Asian ovalocytosis, CR1 deficiency
Pathogenesis:
Sporozoites enter human blood after mosquito bite
↓
Pre-erythrocyticschizogomy in hepatocytes
↓
Cryptozoites released into blood by lysis of hepatocytes
↓
Infection of RBC by cryptozoites
↓
Multiplication within RBC which is converted into schizonts
↓
Lysis of RBC with release of merozoites
↓
Infection of other RBCs
- Hemolysis due to
- Destruction of parasitized RBCs in spleen
- Splenomegaly and activation of hepatosplenic macrophages
- Increased osmotic fragility
- Hemin accumulation
- Oxidative damage to RBC lipids
Clinical features:
- Cold stage (30min-1hr)
- Feeling of chills and rigors
- Nausea and anorexia
- Headache, malaise
- Fever stage (1-4 hrs)
- Intermittent fever, which starts in evening
- Associated with hot flushes and chills and rigors
- Tender hepatosplenomegaly
- Sweating stage (2-3 hrs)
- Temperature falls by crisis
- Profuse sweating
Investigations:
- Identification of parasite in peripheral blood
- Thick smear- For detection of parasite
- Thin smear- For identifying the species
- Serological tests (For histidine rich protein 2 and parasite LDH)
- Species specific card tests are available for vivax and falciparum
- Occasional false positive tests
- Cannot replace microscopy
- Fluorescent microscopy (Quantitative Buffy Coat)
- After staining with acridine orange, RBC containing parasites fluorescence when examined under fluorescent microscopy. False positive tests in case of Howell Jolly bodies and reticulocytes
- PCR: 10 times more sensitive than microscopy
- Hemogram:
- Leucocytosis/ leucopenia
- Monocytosis
- Thrombocytopenia- Seen in almost in every case
Complications:
- Cerebral malaria:
- Seen in severe falciparum malaria
- Occurs due to capillary blockade with perivascular hemorrhage
- Present with fever and coma (which may be preceded by episode of convulsions)
- Can have residual neurological deficits such as hemiplegia, cerebral palsy, cortical blindness, deafness
- Algid malaria:
- Present with vomiting and watery diarrhea leading to hypovolemic shock
- Septic malaria:
- Present with high grade fever, pneumonia and cardiogenic shock
- Black water fever:
- Occurs in falciparummalaria in previously infected patients (hypersensitive state)
- Present with sudden, severe, massive intravascular hemolysis (fever, pain in loin, passage of coco cola colored urine, jaundice, circulatory collapse)
- Tropical splenomegaly
- Occurs due to chronic/ repeated infection
- Can cause pancytopenia
- Treated with lifelong antimalarial prophylaxis. Avoid splenectomy as there is high risk of intra-operative mortality
Treatment:
- Antimalarial agents
- Inj. Artesunate (Falcigo)- 120mg- BD on day 1 and then OD for 3 days (If cerebral malaria, give for 6 days)
- Tab. Chloroquine- 300mg- 2 tablets stat, then 1 tablet after 6 hrs, then OD on day 2 and 3
- Other options: Artemether +Lumefantrine, Sulfadoxine +Pyrimethamine, Quinine, Quinidine, Doxycycline, Mefloquine
- After recovery, for eradicating gametocytes (Pl. Vivax and Pl. Ovale)- Tab. Primaquine- 7.5mg- BD- for 3 days
- Antipyretics for fever
- IV fluids
- Supportive care for cerebral edema, renal failure, convulsions
- Platelet/ PCV as required
- RBC exchange if parasite index is >10% or patient is unconscious
Filariasis
Causative agent:Wucheriabancrofti
Mode of infection:Bite with Culexfatigans
Incubation period: 8-16 months
Pathogenesis:
Infective larva enters skin during bite
↓
Carried by lymphatic system to local lymph node
↓
Larva matures within the lymph node
↓
Lymphangitis due to mechanical irritation, liberation of metabolites which causes lymphatic obstruction
Adult worm releases embryos (microfilaria) into blood stream
↓
Systemic involvement
Clinical features:
- Acute manifestations:
- Fever
- Enlarged regional lymph nodes
- Chronic phase:
- Elephantiasis of limbs and scrotum
- Hydrocele, chyluria, chylous effusion
- Tropical pulmonary eosinophilia
- Low grade fever, loss of weight
- Paroxysmal cough with scanty sputum, dyspnea
- Splenomegaly
- Eosinophilia
- CXR: Diffuse miliary mottling of lung fields
Investigations:
- Demonstration of microfilaria in blood, taken between 9pm and 2am
- Peripheral smear: Microfilariae, eosinophilia
- ELISA for antigen and antibody
- Mazzotti's test: Intense pruritus and rash after administration of DEC
Treatment:
- T. Diethyl carbamazine (DEC)- 250mg- TDS- PO- for 14-21 days
- Plastic surgery for elephantiasis
Kala-azar
Causative agent:Leishmaniadonovani
Mode of infection:Bite of sand fly
Incubation period: 2-6 months
Reservoir of infection: Dogs
Predisposing factors: HIV infection, post transplantation, after immunosuppressive treatment, immunodeficiency states
Pathogenesis:
Promastrigotes injected into human host
↓
Ingested by macrophages and transported to distant organs
↓
Multiplication in reticuloendothelial system
↓
Swollen cell which later ruptures
↓
Released amastigotes again infect other reticuloendothelial cells
Clinical features: (Only 1-3% of infections are symptomatic)
- Fever
- Massive hepatosplenomegaly
- Fatigue due to anemia and wasting
- Lymphadenopathy
- Skin becomes hyperpigmented, rough and dry. Especially skin on forehead, perioral region, nose and temples are affected.
- Post kala-azar dermal leishmaniasis- Hypopigmented skin lesionswhich later form yellowish pink nodules. Commonly seen on extensor surfaces of limbs, sides and back of trunk and besides face.
Investigations:
- Hemogram: Normocytic normochromic anemia, neutropenia, thrombocytopenia (50,000- 1,00,000/cmm)
- DCT- Positive for C3 component and IgG
- BM aspiration
- Hypercellular with panmyelosis
- Lymphocytosis
- Leishman Donovan bodies in macrophages: amastigotes, containing purple nucleus and large anterior kinetoplast
- Similar findings may be noted in aspirates from lymph nodes, liver and spleen
- Prothrombin time- Mildly prolonged due to liver dysfunction
- LFT- Mild increase in bilirubin and transaminases
- Blood culture in Novy-McNeal-Nicolle media
- ELISA- for K39 antigen
- PCR
- Skin biopsy- For demonstration of amastigotes
- Now obsolete tests: Leishmanin test (Intradermal test), Adler test, Napier aldehyde test, Chopra's antimony test, Brahmachari's test
Treatment:
- Antimonials (any one)
- Amphotericin- 1mg/kg/day, until total dose of 20mg/kg
- Liposomal amphotericin B- 3mg/kg/day on days 1-5, and then on days 14 and 21.
- Sodium antimony gluconate- 20mg/kg- IM- OD for 30 days
- PO. Miltefosine- 2-5mg/kg/day
- Inj. Paramomycin- 20mg/kg/day- for 21days
- Antibiotics to prevent secondary infections
Babenosis
Causative agent:
- Babesiamicroti
- Babesiadivergens
Mode of infection:Bite of hard tick
Incubation period: 1-4 weeks
Predisposing conditions: Splenectomised patients, HIV
Pathogenesis:
Inoculation into vertebrate host
↓
Asexual reproduction within RBCs (2-4 parasites per RBC)
↓
Rupture of RBCs causing fever
Clinical features:
- Fever
- Chills
- Muscle pain
- Hemolytic anemia
- Mild hepatosplenomegaly
Investigations:
- Peripheral smear-
- Features of hemolytic anemia
- Maltese cross tetrads within RBCs- Darkly stained ring forms with light blue cytoplasm. No intracytoplasmic pigments
- DCT- Positive for both C3 component and IgG
- Polyclonal hypergammaglobulinemia
- C3, C4 levels- Decreased
- PCR
Complications:
- ARDS
- DIC
- Renal failure
Treatment:
- Most of the infections are self-limited
- Therapy is used for moderate or severe cases only
- Atovaquine + Azithromycin
- Quinine-650mg-TID + Clindamycin- 600mg-TID for 7-10 days
- RBC exchange transfusion if parasitemia is >10%
Bartonellosis
Causative agent:Bartonellabacilliformis
Mode of infection:Bite of sand fly
Pathogenesis:
Infection of RBCs
↓
Parasite attaches to exterior of RBCs
↓
Rapid removal of RBCs by spleen and liver
↓
Hemolysis
Clinical features:2 phases
- Acute hemolytic phase (Oroya fever)
- Fever
- Hemolytic anemia
- Thirst, anorexia, sweating
- Generalized lymphadenopathy
- Chronic granulomatous phase:
- Skin lesions (Verrucaperuviana)- Warty lesions on face and extremities, which bleed later on.
Investigations:
- Peripheral smear- Features of hemolysis, parasites on the surface of RBCs (red violet rods measuring 1-3microns in length)
Treatment:
- Antibiotics: Penicillin, streptomycin, chloramphenicol, tetracyclines
Strongyloidiasis
Causative agent:Strongyloidesstercoralis
Mode of infection:Contact with infected moist soil
Pathogenesis:
Entry of filariform larva into skin
↓
Carried through the blood to right side of heart, then into lungs
↓
Larvae break out of pulmonary capillaries into lung alveoli
↓
Accumulate in sputum and reach intestine when swallowed
↓
Mature and fertilize
↓
Parasitic female lays eggs and rabditiform larvae escape in faeces
Clinical features:
- Skin- Itching at entry site
- Worms in gut- Abdominal pain, diarrhea, steatorrhea, weight loss
- Allergic reaction- Urticaria, wheezing, arthralgia
- Autoinfection through perineal skin- Linear urticarial rashes across abdomen (Larva currens)
- Systemic superinfection (usually occurs in AIDS)
- Diarrhea
- Pneumonia
- Meningo-encephalitis
Investigations:
- Stool microscopy- Larvae are seen
- Sputum microscopy- Larvae can be seen
- Jejunal aspiration
- Serology by ELISA
Treatment:
- T. Levamisole
Figures:
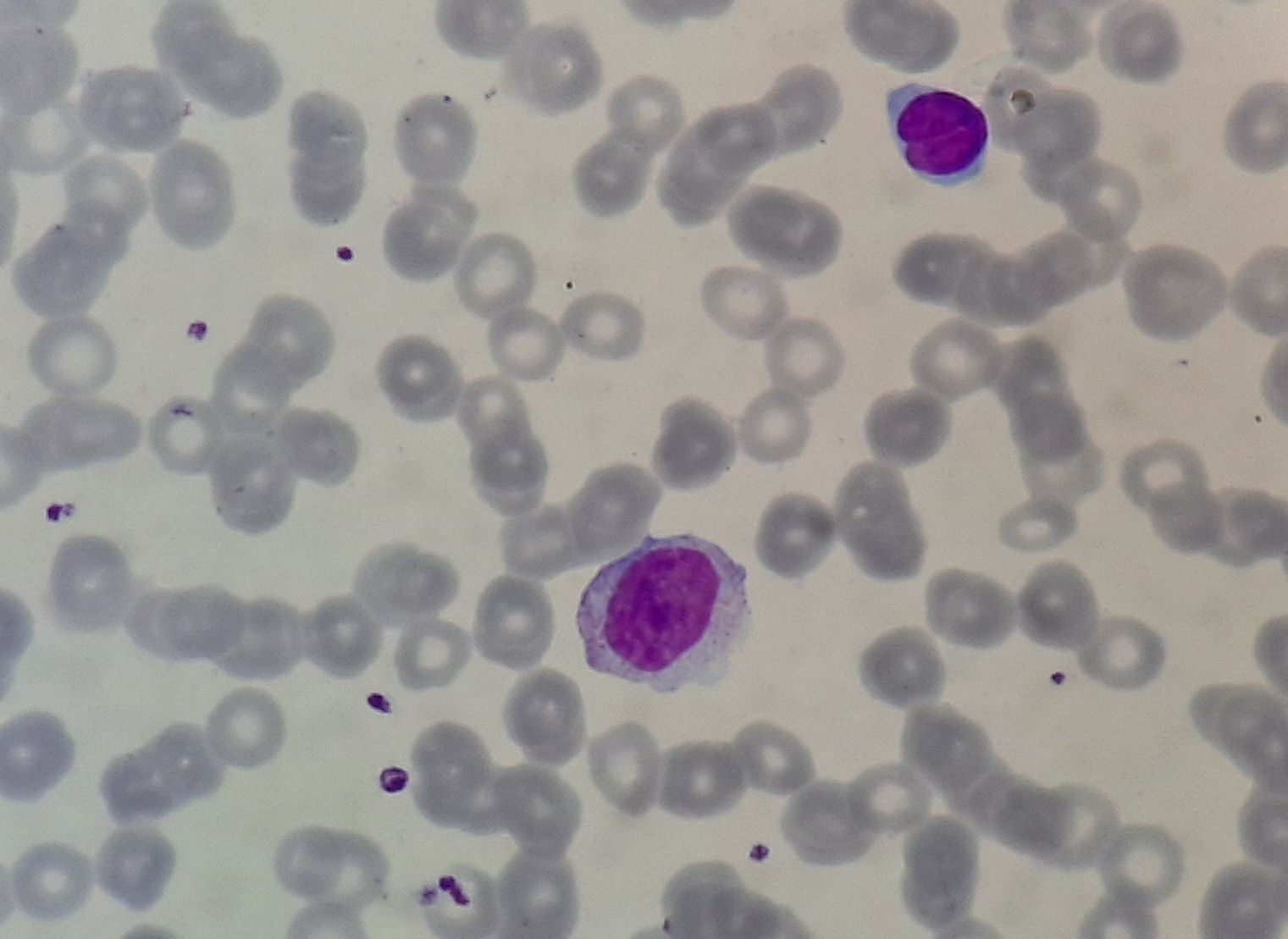
Figure 11.20.1- Reactive lymphocyte in infectious mononucleosis
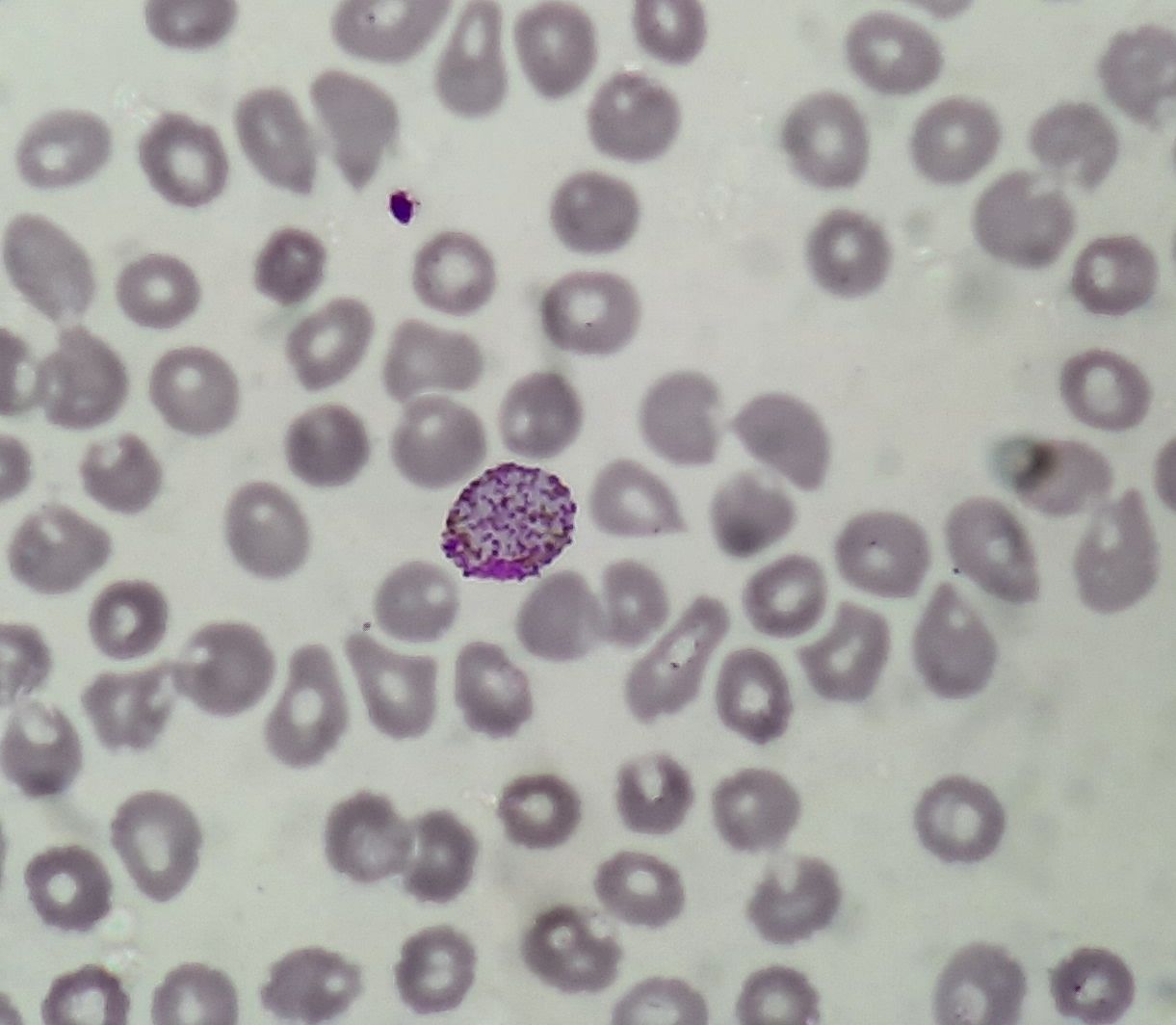
Figure 11.20.2- Malarial parasite in peripheral smear
Recent advances:
Automated production of specific T cells for treatment of refractory viral infections after allogeneic stem cell transplantation
This study focuses on adoptive cellular therapy using virus-specific T cells (VST) for therapy-resistant viral reactivations after hematopoietic stem cell transplantation. The authors employed the CliniMACS Prodigy® system for closed-system production of VST, ensuring scalability. They assessed the therapy's efficacy in 26 patients with various viral diseases (adenovirus, cytomegalovirus, Epstein-Barr virus, multi-viral). VST production was successful in all cases, and safety was favorable, with reversible adverse events in a few patients. A 77% response rate was observed, correlating with better overall survival compared to non-responders. Virus-specific symptoms improved in nearly half of the patients, and the 6-month overall survival for the cohort was 28%.
https://doi.org/10.3324/haematol.2022.281996
Adoptive therapy with cytomegalovirus-specific cytotoxic T lymphocytes for refractory cytomegalovirus DNAemia and disease after allogeneic haematopoietic stem cell transplantation
In a retrospective study comparing the efficacy and safety of donor and third-party CMV-specific cytotoxic T lymphocytes (CMV-CTLs) in patients with refractory CMV DNAemia or disease after allogeneic hematopoietic stem cell transplantation (allo-HSCT), 53 adult patients were enrolled. Within 6 weeks of treatment, similar proportions of patients achieved complete response in both groups. The 2-year overall survival rates did not significantly differ between the donor and third-party groups. Acute graft-versus-host disease occurred in a small proportion of patients in both groups. These findings suggest that donor and third-party CMV-CTLs exhibit comparable efficacy and safety for treating refractory CMV DNAemia and disease after allo-HSCT.
https://doi.org/10.1111/bjh.19282
Letermovir prophylaxis reduced cytomegalovirus reactivation and resistance post umbilical cord blood transplantation
In this retrospective study comparing umbilical cord blood transplantation (UCBT) patients receiving letermovir (LET) prophylaxis to a historical cohort without LET, LET administration significantly reduced the 180-day cumulative incidence of cytomegalovirus (CMV) reactivation (47.3% vs. 74.4%, p < 0.001) and refractory CMV reactivation (15.0% vs. 42.9%, p = 0.016). However, LET prophylaxis was associated with a higher incidence of late CMV infection (31.0% vs. 4.3%, p = 0.002) and a trend towards increased Epstein–Barr virus (EBV) reactivation (9.3% vs. 3.4%, p = 0.087). Older age (>15 years) and pre-engraftment syndrome were identified as significant risk factors for CMV reactivation, with LET demonstrating greater benefit in high-risk patients (46.7% vs. 86.5%, p < 0.001) compared to low-risk patients (47.8% vs. 62.1%, p = 0.120).
https://doi.org/10.1111/bjh.19451
Infection risk and antimicrobial prophylaxis in bendamustine-treated patients with indolent non-Hodgkin lymphoma
This multicenter retrospective study analyzed infections and antimicrobial prophylaxis in 302 bendamustine-treated indolent non-Hodgkin lymphoma patients. Lymphopenia was nearly universal, but its severity and duration were not associated with infection risk. Infections occurred in 44% of patients, with 27% hospitalized, and 32% of infections happened more than three months post-treatment. Opportunistic infections were noted, including varicella zoster virus (VZV) and Pneumocystis jiroveci pneumonia (PJP). Prophylaxis reduced the risk of VZV/HSV and bacterial infections, highlighting the importance of prophylaxis in managing infection risks.
https://doi.org/10.1111/bjh.19407
HHV-6 related mortality after hematopoietic cell transplant
This systematic review and meta-analysis assessed the impact of HHV-6 reactivation on mortality following allogeneic hematopoietic stem cell transplant. Reactivation was significantly associated with increased non-relapse mortality and overall mortality. Bayesian analysis confirmed the findings for NRM, while OM results showed some heterogeneity (I² = 36.7%). These findings suggest that HHV-6 detection contributes to poorer outcomes post-HCT. Randomized trials are needed to determine if strategies to prevent or treat HHV-6 reactivation can improve patient survival.
https://doi.org/10.1038/s41409-024-02398-w
Risk and impact of cytomegalovirus infection in lymphoma patients treated with bendamustine
In this retrospective study of 211 lymphoma patients treated with bendamustine, clinically significant CMV infection (CS-CMVi) occurred in 12.8% and was associated with higher mortality. Risk factors for CS-CMVi included prior lines of therapy (≥1), hypoalbuminemia (<3.5 g/dL), and liver disease. The cumulative incidence was 10.1 per 100 person-years over three years. CS-CMVi highlights the need for careful monitoring in at-risk patients.
https://doi.org/10.1007/s00277-024-05839-0
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.