
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
Immune deficiency and dysregulation associated lymphomas
This category includes includes:
- LPDs Associated with inborn errors of immunity
- Post-transplant lymphoproliferative disorders
- Iatrogenic immunodeficiency associated lymphoproliferative disorders
- HIV associated lymphomas
Lymphoid proliferations and lymphomas associated with immune deficiency and dysregulation include: (Common to all)
- Hyperplasias arising in immune deficiency/dysregulation (Most of them are EBV related)
- Follicular proliferations:
- Follicular hyperplasia
- Follicle lysis/ involution
- Lymphoid/ lymph node depletion
- Progressive transformation of germinal center
- Castleman disease like changes
- Interfollicular and paracortical proliferations
- Infectious mononucleosis-like hyperplasia
- Plasmacytic hyperplasia
- Other types of hyperplasias and involutions
- EBV reactivation
- Immune reconstitution inflammatory syndrome
- T cell and histiocytic proliferations
- Hemophagocytic lymphohistiocytosis
- Extranodal T cell proliferation/ expanstion especially ALPS
- Chronic active EBV disease
- Follicular proliferations:
- Polymorphic lymphoproliferative disorders arising in immune deficiency / dysregulation
- Polymorphic lymphoproliferative disorder
- EBV+ mucocutaneous ulcer
- KSHV/HHV8-positive germinotropic lymphoproliferative disorder
- Lymphomas arising in immune deficiency / dysregulation
- Small (low grade) B cell lymphomas
- Diffuse large B-cell lymphoma
- Burkitt lymphoma
- Classical Hodgkin lymphoma
- KSHV/HHV8+ diffuse large B-cell lymphoma, NOS
- Primary effusion lymphoma
- Plasmablastic lymphoma
- Plasma cell neoplasms
- T- and NK- cell lymphomas
3 part nomenclature used for LPDs associated with immune deficiency and dysregulation:
Name of diagnosis must include: Name of lesion, virus status, type of immunodeficiency
Examples:
- Follicular hyperplasia, EBV+, HIV setting
- Burkitt lymphoma, EBV-, posttransplant setting
- Classic Hodgkin lymphoma, EBV+, HIV setting
- Extranodal marginal zone lymphoma, EBV-, hyper-IgM syndrome
LPDs associated with inborn errors of immunity
Introduction:
- As IEIs are heterogeneous, LPDs are also highly variable
- Most common type of LPD in IEI is diffuse large B-cell lymphoma
- IEIs most commonly associated with LPDs
- Ataxia telangiectasia
- Wiskott Aldrich syndrome
- Common variable immunodeficiency
- Severe combined immunodeficiency
- X-linked immunoproliferative disorders
- Nijmegen breakage syndrome
- Hyper IgM syndrome
- Autoimmune lymphoproliferative disorder
Risk Factor: EBV Infection
Classification:
- B-cell neoplasms
- Diffuse Large B-cell Lymphoma
- Lymphomatoidgranulomatosis
- Burkitt lymphoma
- T-cell Neoplasms
- Precursor T lymphoblastic lymphoma / leukemia
- T-cell prolymphocyticleukemia
- Hodgkin’s Lymphoma
Prognosis: Depends on type of LPD and underlying IEI
Treatment:
- Lymphoma specific chemotherapy: Generally less aggressive therapy, than patients without IEI is needed.
- Radiotherapy should be avoided in patients with DNA repair defects
- Allo SCT may be curative, both for lymphoma and IEI
Post-transplant Lymphoproliferative Disorder
Categories of post-transplant lymphoproliferative disease (PTLD)
- Non-destructive/Early lesions
- Infectious mononucleosis like- Paracortical expansion and numerous immunoblasts in background of small lymphocytes
- Reactive plasmacytic hyperplasia- Polytypic light chain staining
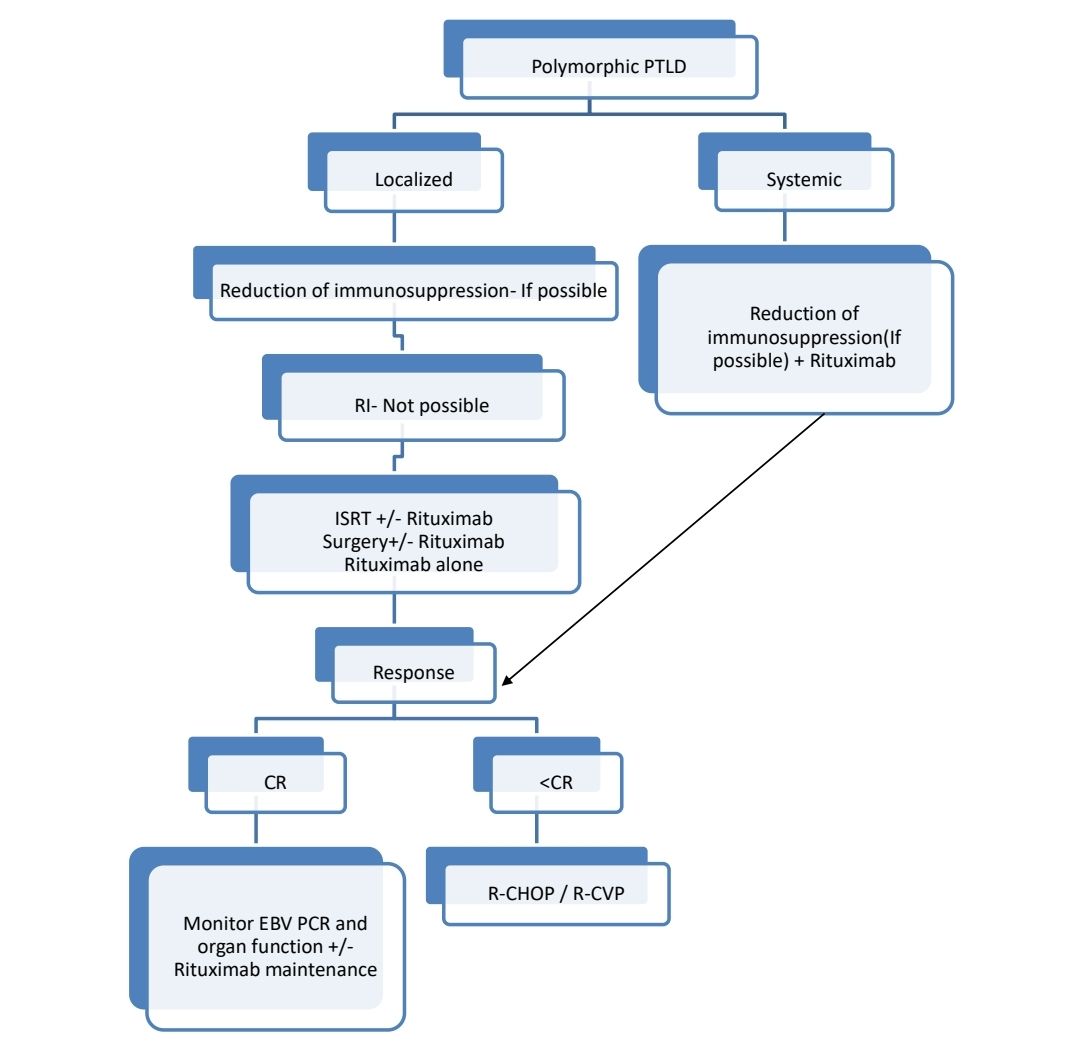
- Polymorphic PTLD- Destructive lesions composed of immunoblasts, plasma cells, and intermediate sized lymphoid cells that efface lymph node architecture or form destructive extra nodal masses
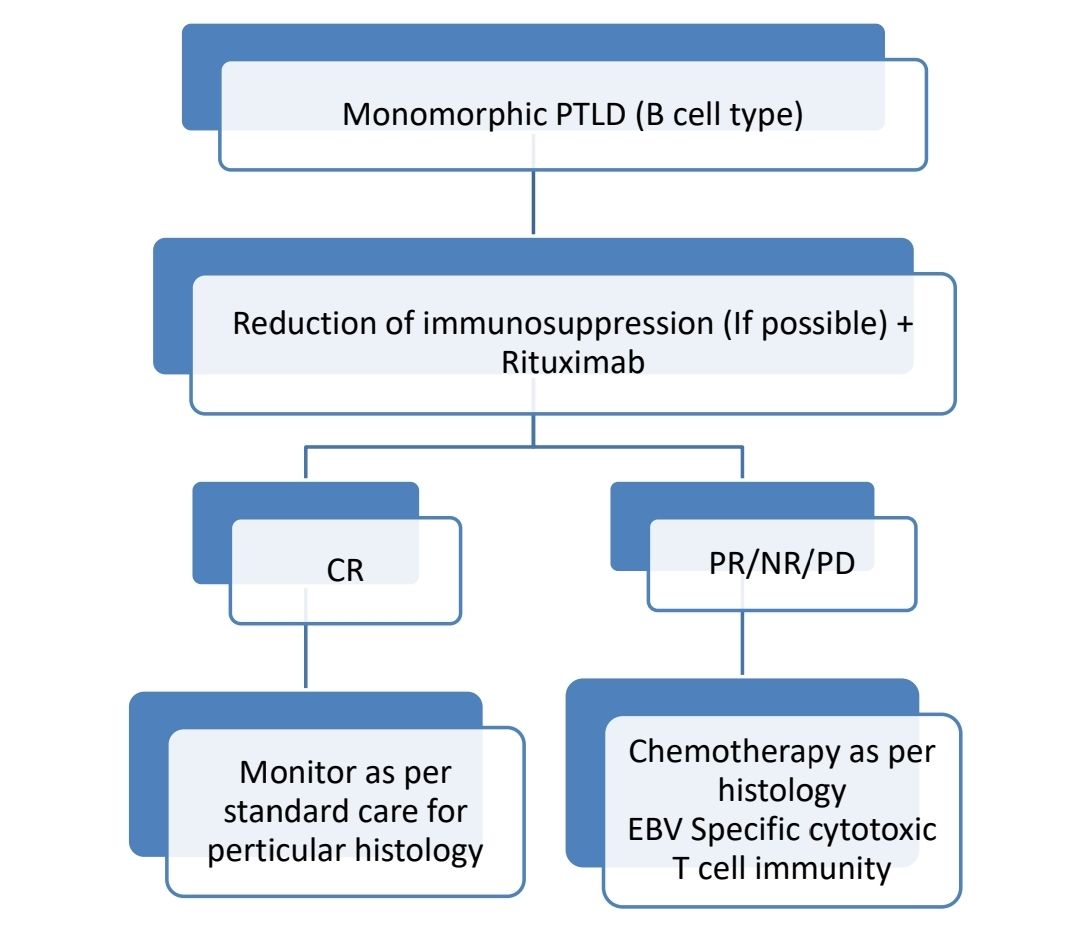
- Monomorphic PTLD
- B-cell neoplasms
- Diffuse large B-cell lymphoma (immunoblastic, centroblastic, anaplastic)
- Burkitt / Burkitt-like lymphoma
- Plasma cell myeloma
- Plasmacytoma like lesions
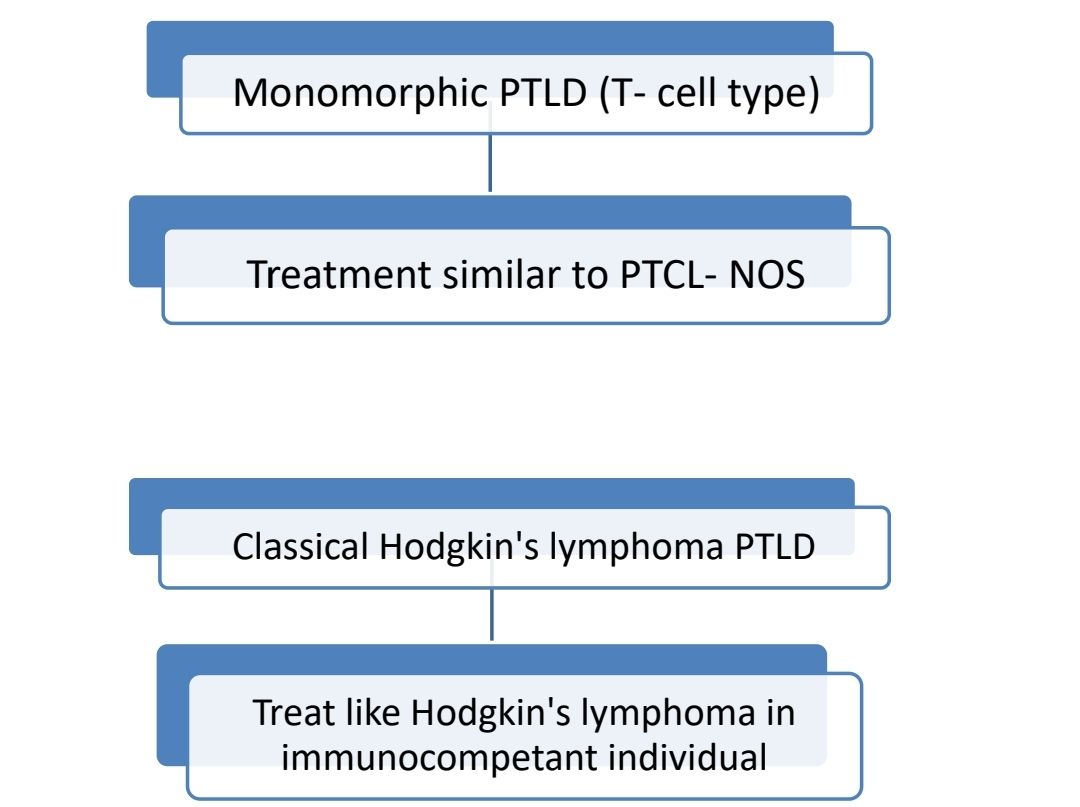
- T-Cell neoplasms
- Peripheral T-cell lymphoma, not otherwise specified
- Other types of NK, T cell lymphomas
- B-cell neoplasms
Risk
- Bone marrow transplant- <1%
- Renal transplant - <1%
- Hepatic, cardiac – 1-2%
- Heart lung, liver, bowel – 5 %
- Immunosuppression for GVHD – 20%
Etiology:
- EBV
- Use of Azathioprine / Cyclosporin / Tacrolimus
- Risk factors in stem cell transplant
- T cell depletion allograft
- Unrelated or HLA mismatched grafts
- Anti T cell therapy for GVHD
- Higher recipient age
- Risk factors in solid organ transplant:
- Type of organ transplant: High risk with bowel and lung
- CMV/EBV positive donor
- HLA mismatch
- Anti T cell therapy
Clinical Features:
- Lymphadenopathy
- Hepatomegaly/ splenomegaly
- Extranodal involvement is common with solid organ transplants
- B symptoms
Investigations:
- Histopathology
- Immunophenotyping by IHC
- Imaging for staging
- EBER in situ hybridization
Prognosis:
- Overall mortality- 50%
- Poor prognostic markers
- Poor performance score
- EBV negative tumor
- Graft organ involvement
- Monomorphic pathology
Pretreatment Work-up:
- History
- B-Symptoms
- Immunosuppression
- Examination
- LN:
- Spleen:
- WHO P. S.
- BSA
- IHC
- BMA and Bx
- CT (CAP)/ PET
- Stage
- Hemoglobin
- TLC, DLC
- Platelet count
- LFT: Bili- T/D SGPT: SGOT: Albumin: Globulin:
- Creatinine
- Electrolytes: Na: K: Ca: Mg: PO4:
- Uric acid:
- LDH
- HIV:
- HBsAg:
- HCV:
- EBV PCR
- CMV PCR
- UPT
- ECHO (If anthracyclines planned) LVEF- %
- Chemotherapy consent after informing about disease, prognosis, cost of therapy, side effects, hygiene, food and contraception
- Fertility preservation
- PICC line insertion and Chest X ray after line insertion
- Tumor board meeting and decision
- Attach supportive care drug sheet
- Inform primary care physician
Treatment Plan:
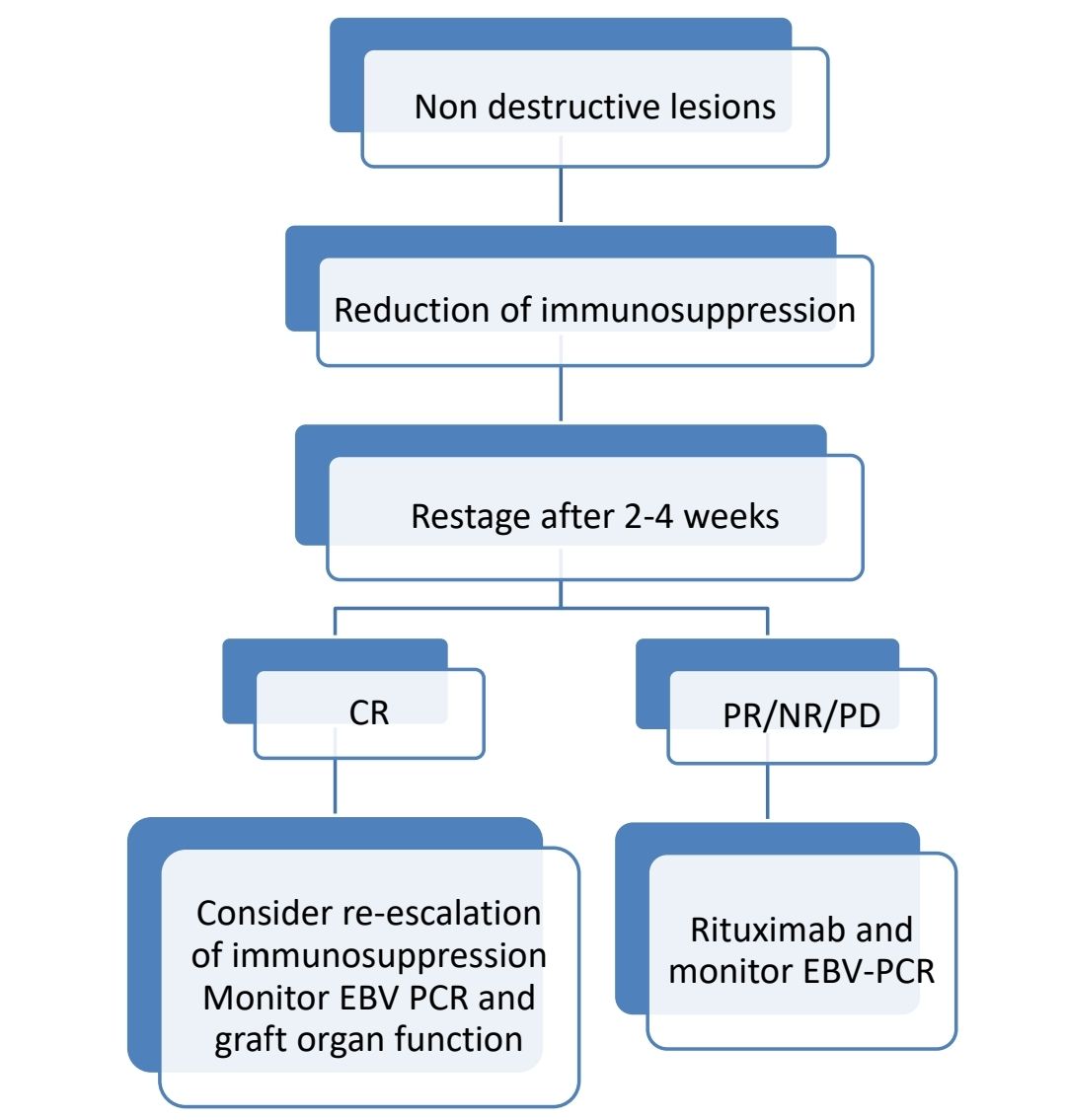
Reduction in immunosuppression:
- Response to RI is variable
- It should be co-ordinated with transplant team
- Reduce calcineurin inhibitor to about 50% (Cyclosporine and tacrolimus)
- Discontinueantimetabolic agents (Azathioprine and MMF)
- For critically ill, all non-glucocorticoidimmunosuppression must be stopped.
- Stopping immunosuppression completely is feasible only if
- Alternate support is available- Ex: Dialysis for renal transplant
- Transplanted organ is resistant to rejection. Ex: Liver
- Response to RIS is assessed by
- Assessing change in tumour size
- Reduction in LDH
- Resolution of constitutional symptoms
- Response is often seen in 2-4 weeks.
- If there is graft rejection, retransplantation can be done after PTLD has been treated. There are good results with retransplantation. Retransplantation should be done 1 year after control of PTLD.
Iatrogenic Immunodeficiency Associated Lymphoproliferative Disorders
- They include lymphomas that arise in patients treated with immunosuppressive drugs for autoimmune diseases or conditions other than the allograft/ autograft transplant setting.
- They include
- Polymorphic lesions that are seen in post transplant LPDs
- DLBCL
- T/NK cell lymphoma
- Classical Hodgkin's lymphoma
- Etiology: Methotrexate, Infliximab, Adalimumab, Etanercept
- EBV is seen in 40% of cases.
- Survival depends on type of LPD.
- Many show at least partial regression after stopping drug.
- Others need chemotherapy
HIV Associated Lymphoma
- Lymphomas seen in HIV patients include
- DLBCL
- Burkitt’s lymphoma
- MALT lymphoma
- Plasmablastic lymphoma of oral cavity
- Primary effusion lymphoma
- Hodgkin’s lymphoma
- Peripheral T cell lymphoma
- KSHV/HHV8+ multicentric castleman disease
- Primary CNS lymphoma
- Incidence of lymphoma in HIV patients is 60-200 times more than general population
- Causes:
- Infection with EBV
- Infection with Kaposi’s sarcoma human virus
- Chronic antigenic stimulation
- Genetic abnormalities
- Cytokine dysregulation due to increased serum levels of IL6 & IL10
- Abnormalities involving MYC and BCL-6 oncogenes
- Pathogenesis:
1.
HIV Infection
Ongoing infections
↓
Macrophage activation with release of cytokines
Chronic antigenic stimulation
↓
Proliferation of B lymphocytes
↓
Recombinase error
↓
Abnormal DNA rearrangements
↓
Chromosomal abnormalities
↓
Mutations in critical oncogenes or tumor suppressor genes
↓
Clonal selection
↓
Development of lymphoma
2.
Compromised cellular immunity
↓
Decreased immune surveillance of EBV and KSHV infected B cells
↓
Viral lymphomagenesis
- Prognosis:
- Outcome of therapy is same as non-HIV cases, when chemotherapy is combined with HAART therapy
- Poor prognostic markers
- CD4 count of <200/cmm
- Age prognostic markers
- IV drug use
- Stage III/IV disease
- Plasmablastic lymphoma has aggressive disease with survival of <1 year
- Pretreatment workup
- History including B-Symptoms
- Examination
- LN:
- Spleen:
- WHO P. S.
- BSA
- IHC
- Subtype
- BMA and Bx(Can avoid if PET Negative)
- CT (CAP)/ PET
- Stage
- Hemoglobin
- TLC, DLC
- Platelet count
- LFT: Bili- T/D SGPT: SGOT: Albumin: Globulin:
- Creatinine
- Electrolytes
- Uric acid:
- LDH
- Beta 2 Microglobulin
- CD4 count
- HIV Viral Load
- LP (Except for early DLBCL and Primary Effusion Lymphoma)
- HBsAg:
- HCV:
- UPT
- ECHO(If anthracyclines planned)- LVEF
- Treatment
- ART has to be initiated/ continued during the chemotherapy as well. Avoid using zidovudine, cobicistat and ritonavir, as they tend to increase drug toxicity.
- All must receive PCP and other prophylaxis
- If CD4 count <50/cmm, maximise supportive care and monitor closely for cytopenias and infections
- If CD4 count <100, avoid Rituximab
- Give G-CSF for all patients
- Give CNS prophylaxis for all category of patients (By intrathecal therapy)
- Treatment is similar to immunocompetent patients
- For DLBCL, HHV-8 positive DLBCL, Primary effusion lymphoma- R-EPOCH is preferred over R-CHOP.
- For plasmablastic lymphoma- R-CHOP is not adequate therapy. Give EPOCH or CODOX-M/IVAC or Hyper-CVAD followed by HDT and ASCR in CR1.
- For non-Burkitt lymphomas, when EPOCH is being used following adjustments must be made:
- Etoposide, Vincristine and Doxorubicin must be infused over 96 hrs
- Dose of Day 5 Cyclophosphamide is reduced to 187.5mg/m2, if CD4 count is <50/cmm
Recent advaces:
Outcomes of HIV-Associated High-Grade B-Cell Non-Hodgkin Lymphoma (NHL) Treated with Dose Adjusted EPOCH (+/−R) Regimen
In a retrospective analysis of treatment-naïve HIV-associated high-grade B-cell non-Hodgkin lymphoma (NHL) patients aged 18 and above treated with the DA-EPOCH(+/-R) regimen from 2011 to 2015, a cohort of 40 patients was studied. The cohort included diffuse large B-cell lymphoma (DLBCL), Burkitt’s lymphoma, high-grade B-cell lymphoma-unclassifiable, and plasmablastic lymphoma. The median CD4+ T cell count was 202/mm3, and CNS prophylaxis was administered to 90% of patients. With a median follow-up of 72 months, the estimated 5-year overall survival (OS) was 82.5%, and 5-year progression-free survival (PFS) was 77.5%. At least 4 cycles of chemotherapy were administered to 93% of patients. Grade 3–4 toxicities were observed in 83% of patients, with febrile neutropenia being the most common.
https://doi.org/10.1007/s12288-023-01652-3
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.