
howitreat.in
A user-friendly, frequently updated reference guide that aligns with international guidelines and protocols.
Marginal Zone Lymphoma (EMZL, MALToma, PCMZL, NMZL, IPSID)
Updated on 20.02.2025
Introduction:
- These are a group of clinically indolent mature B-cell lymphomas derived from memory B cells of the ‘marginal’ zones of secondary lymphoid tissues.
- This category includes following disorders:
- Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (EMZL/MALT)
- Gastric (30-40%)
- Non-gastric(60-70%): Other sites in GIT, Lung, ocular adnexa, thyroid, breast, small intestine, salivary gland, skin, breast and thymus
- Primary cutaneous marginal zone lymphoma (PCMZL)
- Nodal marginal zone lymphoma (NMZL)
- Pediatric nodal marginal zone lymphoma (PNMZL)
- Immunoproliferative small intestinal disease (IPSID) is also considered as a type of MALT lymphoma
- Splenic marginal zone lymphoma is now classified under: Splenic B Cell lymphoma and leukemias
- Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (EMZL/MALT)
- CNS involvement is rare
Epidemiology:
- Account for 15% of all NHL
- 3rd most common lymphoma (After DLBCL and FL)
Etiology:
- Often seen in the context of chronic infection or autoimmune disease
Pathogenesis:
Chronic inflammation Ex: H. Pylori infection
↓
Activation of B lymphocytes
↓
Acquisition of molecular lesions in pathways that were previously activated by the inflamed microenvironment
(B-cell receptor, NF-κB, and NOTCH)
↓
Transformed B cell is no longer dependent on the microenvironment
In addition: translocations involving the immunoglobulin heavy-chain locus
(IGH) on chromosome 14 — t(1;14) and t(14;18)à up-regulation of BCL10 and MALT1, respectively
TET2 mutations block B-cell differentiation into plasma cells
↓
Development of marginal zone lymphoma
- Histological transformation is driven by TP53 mutations, loss of p16 protein, or rearrangements in MYC
Clinical features:
- Depends on the type of MZL and organ involved
Immunohistochemistry:
- Neoplastic cells are small mature B cells
- They are positive for: CD20, BCL2, BCL6, CD21
- They are negative for CD5, CD10, CD23, LEF1, Cyclin D1, SOX11, IgD
- Ig light chain restriction is present
- Variable: CD43
- Plasmacytic differentiation is often present
- Reactive follicles are often present
Prognosis:
- Usually have indolent course
- Strongest poor prognostic marker: Progression of disease within 2 years after initial treatment
- Incidence of transformation to aggressive large B-cell lymphoma of 4.7% at 10 years
Pretreatment Work-up (Applicable for all subtypes of MZL. For additional tests refer individual disease sections):
- History
- B-Symptoms
- Examination
- LN:
- Spleen:
- WHO P. S.
- BSA
- IHC
- Hemoglobin
- TLC, DLC
- Platelet count
- Peripheral smear
- LFT: Bili- T/D SGPT: SGOT: Albumin: Globulin:
- Creatinine
- Electrolytes: Na: K: Ca: Mg: PO4:
- Uric acid:
- LDH
- Beta-2- microglobulin
- Protein electrophoresis
- HIV:
- HBsAg and core antibody
- HCV: (if positive for HCV, PCR test for HCV RNA and viral genotyping; cryoglobulins and cryocrit)
- BMA and Bx: If there is associated cytopenia
- CECT (NCAP) / PET-CT (PET should be done if there is suspicion of high grade transformation or if disease is localized and hence RT is being planned)
- Stage
- UPT
- ECHO (If anthracyclines planned) LVEF- %
- Chemotherapy consent after informing about disease, prognosis, cost of therapy, side effects, hygiene, food and contraception
- Fertility preservation
- PICC line insertion and Chest X ray after line insertion
- Tumor board meeting and decision
- Attach supportive care drug sheet
- Inform primary care physician
Treatment:
- Treatment is planned based on:
- Type of MZL
- Site and stage of disease
- Whether tumor can be surgically excised
- Ease of administering locoregional ISRT
- For limited stage disease:
- Site specific antibiotic therapy must be given especially if PCR is positive.
- If antibiotic cannot be given/ does not work, radiation therapy next choice.
- Surgical excision may be considered for MALTomas involving lung, breast, thyroid, colon/small bowel
- For refractory/ relapsed early stage disease: Treatment same as advanced stage disease
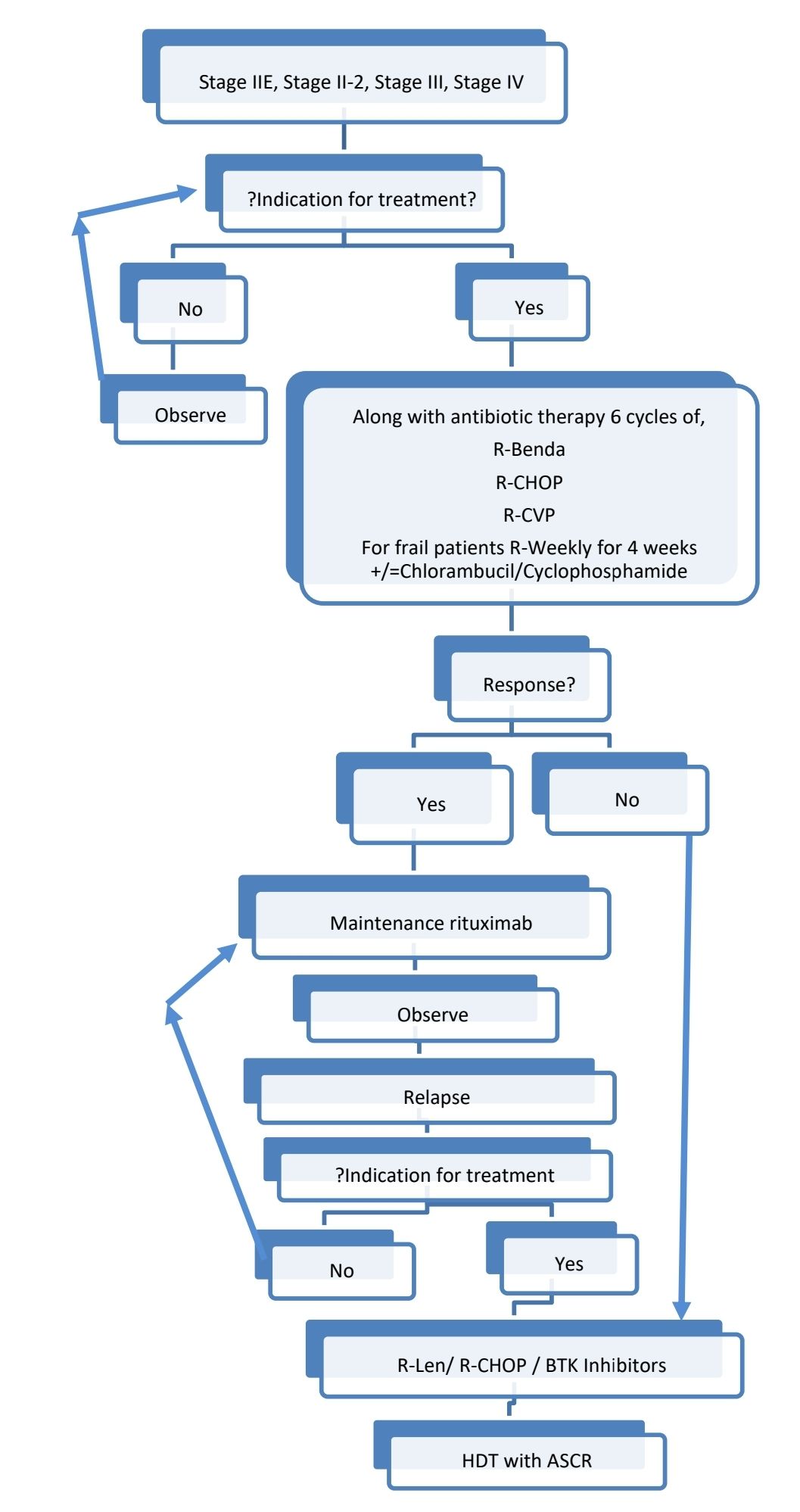
- For advanced stage disease (Stage II,III and IV):
- Treat only if indication for treatment are present
- Chemotherapy with Rituximab
- Consider maintenance rituximab after achieving CR/ PR
- For relapsed disease
- RT for localized relapse
- BR/ other chemotherapy, if not used so far
- BTK inhibitors
- Lenalidomide- Rituximab
- Tafasitamab, an anti-CD19-directed humanised monoclonal antibody
- CAR-T cell therapy: axicabtagene ciloleucel
- Autologous stem cell transplantation in selected patients (fit)
- Disease with high grade transformation is treated similar to DLBCL
Response assessment:
- Must be done after 3-6 months of therapy
- Includes: History, examination, CBC, BM (if previously involved) and CT (Neck, chest, abdomen and pelvis)
Gastric extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue
(Gastric MALT lymphoma)
Introduction:
- It is an indolent, primary extranodal B-cell lymphoma arising from gastric mucosa-associated lymphoid tissue.
- Cell of origin is marginal zone B cell
- Often associated with an underlying infection associated chronic gastritis
Epidemiology:
- 50% of primary gastric lymphoma
- Median age- 61 years
- Slight female preponderance
Etiology:
- H. pylori gastritis
- H. heilmannii associated gastritis
Clinical Features:
- Dyspepsia
- Reflux esophagitis
- Abdominal pain
- Nausea
- Weight loss
Complication:
- Transformation into DLBCL
Investigations:
- Upper GI scopy
- Erythema/ erosions/ ulcers/ masses
- Multiple biopsies of suspicious areas must be taken
- Endoscopic biopsy
- Lymphoma cells infiltrate around reactive B-cell follicles, external to preserved follicle mantle, in a marginal zone distribution and spread out to form larger confluent areas which eventually over run most of the follicles.
- Marginal zone B cells are small to medium sized. Their nuclei are slightly irregular with moderately dispersed chromatin and inconspicuous nucleoli. Cytoplasm is abundant and pale (Monocytoid appearance). Sometimes Plasmacytic differentiation is present (1/3rd cases)
- Larger cells resembling centroblasts or immunoblasts are usually present.
- Lympho epithelial lesions- Aggregates of 3 / more marginal zone cells with distortion of the epithelium, often together with eosinophilic degeneration of epithelial cells
- Immunophenotyping by immunohistochemistry
- Positive- Immunoglobulin light chain restriction, IgM, CD20, CD79a, PAX5, dim-moderate- CD11c , Marginal zone associated antigens (CD21, CD35)
- Negative- CD5, CD23, CD10, CD103, Cyclin D1, SOX11, aberrant CD43 and TBX21 (T- bet)
- H. Pylori testing
- Biopsy
- Urea breath test
- BM examination- Involved in 10% of cases
- S. LDH- Increased in advanced stages
- SPE: M band may be detected
- S. Beta 2 microglobulin- Increased in advanced stages
- CT scan- Chest, abdomen, pelvis
- Endoscopic ultrasound- To evaluate regional lymph nodes and gastric wall infiltration
- Molecular studies:
- Antigen receptor genes- Rearrangement and mutations in Ig light and heavy chain genes, in variable region, consistent with derivation from post germinal centre memory B cell
- Cytogenetics
- Trisomy 3 and 18
- t (11 : 18) – Fusion of API2 with MLT leading to activation of NFk beta. It is present in 40% cases and is associated with failure to respond to eradication of H. Pylori.
- del 6q23 involving TNF-AIP-3
- FISH Panel
- t (1:14)
- t (3:14)
- t (11:14)
- t (11:18)
- t (14:18)
Criteria for diagnosis:
Essential:
- Primary ymphoma arising in an extranodal site.
- Atypical small/medium-sized lymphoid cell proliferation mimicking reactive MALT and showing architectural distortion.
- Expression of B-lineage markers.
- Exclusion of other small B-cell neoplasms, e.g., follicular lymphoma, mantle cell lymphoma, small lymphocytic lymphoma, lymphoplasmacytic lymphoma and plasmacytoma.
Desirable:
- Demonstration of light chain restriction or clonal immunoglobulin gene rearrangement.
- Lymphoepithelial lesions.
- Remnants of underlying inflammatory background e.g., reactive lymphoid follicles, Hashimoto thyroiditis in thyroid or lymphoepithelial sialadenitis in salivary gland.
Staging: Lugano staging system for GI lymphomas
- Stage I- Confined to GI tract (I1- Mucosa, submucosa, I2- Muscularis propria, serosa )
- Stage II- Extending into abdomen (II1- Local nodal involvement, II2- Distant nodal involvement)
- Stage IIE- Penetration of serosa to involve adjucent organs or tissues
- Stage IV- Disseminated extranodal involvement or concomitant supradiaphragmatic nodal involvement. Or bone marrow involvement
Prognosis:
- Indolent course
- 10 year survival: 80%
- EMZL/MALT international prognostic index (Useful for gastric and non-gastric EMZL/MALT). Factors included are:
- Age >70 years
- Ann Arbor stage III/IV
- Elevated LDH
Risk factors | 5 year event free survival |
0 | 70% |
1 | 56% |
≥ | 29% |
Indications for Treatment:
- Symptomatic patients
- GI bleeding
- Threatened end organ function
- Bulky disease
- Steady/ rapid progression
- Patient preference
Additional tests in pretreatment work up
- H. Pylori Stain on gastric biopsies
- Urea Breath/ Stool Antigen (For HP Stain -ve Cases)
- FISH for t(11;18) and fusion of BIRC3 (formerly API2) and MALT1 (Positive cases generally do not respond to H. Pylori eradication treatment)
- Oesophago-gastro- duodenoscopy ± endoscopic ultrasound with high-quality photography and a detailed description of the site of lesions
Treatment Plan:
Limited stage disease:
- Stage I, II-1, H. Pylori- Positive, t (11:18) Negative/ Unknown- Antibiotic therapy for H. Pylori
- Stage I, Stage II-1, H. pylori-Positive, t(11:18)-Positive- Antibiotic therapy + IFRT (Rituximab if ISRT is contraindicated)
- Stage I, Stage II-1, H.Pylori- Negative- ISRT (Rituximab if IFRT is contraindicated)
Advanced stage disease:
Large cell transformation of MALToma, has to be treated like DLBCL.
About Each Modality of Treatment:
- H. Pylori eradication: Includes PPI with following antibiotics for 14 days
- 1st line:
- Clarythromycin- 500mg- BD
- Amoxycillin- 1000mg- BD
- 2nd line
- Metronidazole- 500mg- 1-1-1
- Tetracycline- 500mg- QID
- Bismuth subcitrate- 120mg- QID
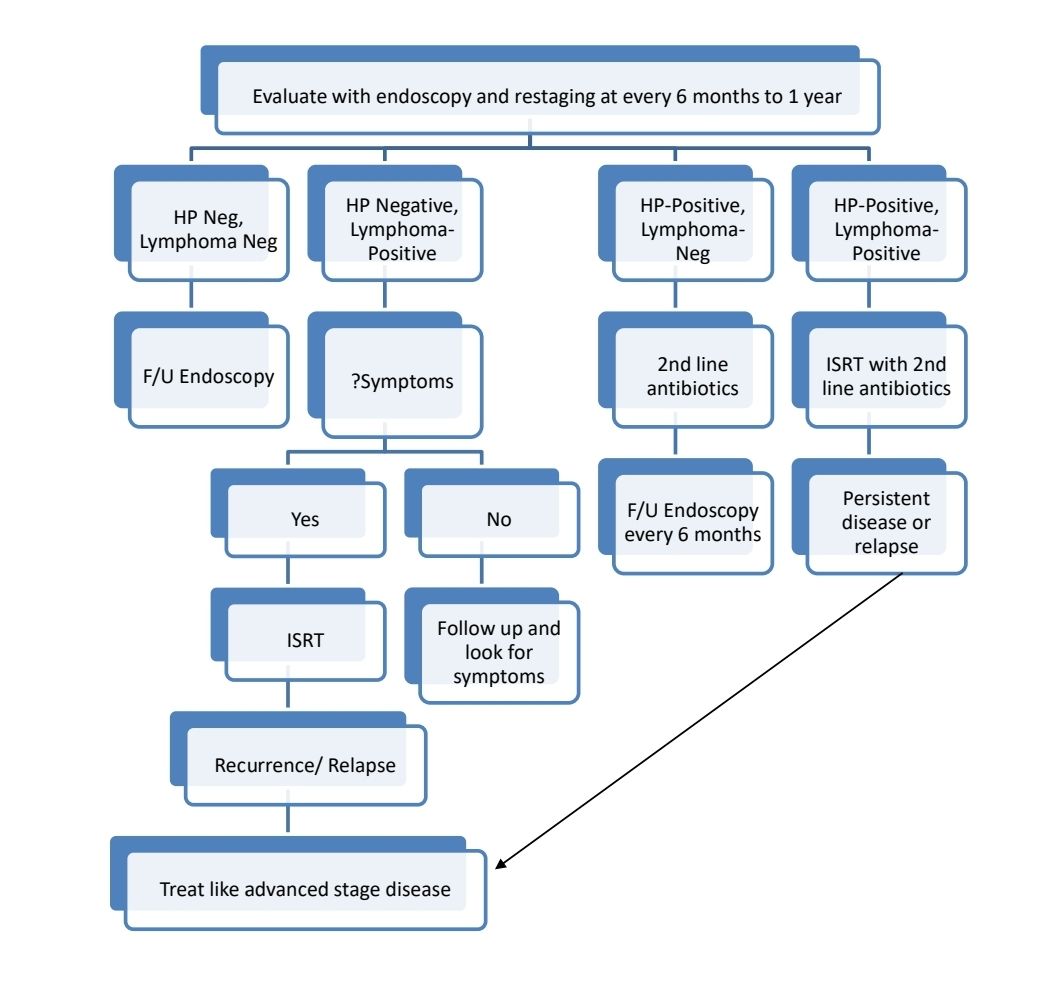
- Reassessment must be done at 6 months to 1 year
- About 60% achieve CR at 1 year
- 1st line:
- Radiotherapy:
- 30-40 Gy given over 4 weeks
- Adjacent nodes should be included
- Chemotherapies:
- Must be combined with H. pylori eradication
- Better to give maintenance rituximab, 375 mg/m2 every 8 weeks for up to 12 cycles.
- Note: Gastrectomy results in significant morbidity and has not been shown to achieve superior results in comparison to organ preserving strategies.
Monitoring After Treatment/ Follow-up:
- If treated with antibiotics alone: stool antigen test or urea breath test ≥6 weeks after starting eradication
- Repeat endoscopy twice a year for 5 years
- Then once a year/ as clinically indicated
MALT lymphoma of Ocular adnexa
Etiology:
- Chlamydia psittasi
Additional evaluations:
- CT or MRI orbits, head and neck
- Ophthalmology examination with photodocumentation
- PCR for C. psittaci on tumour biopsy or conjuctival swab or peripheral blood mononuclear cells
- Peripheral blood mononuclear cells
- Anti-SSA and anti-SSB antibodies
Treatment of early stage disease:
- First-line antibiotic regimen: Doxycycline 100 mg BD for 21 days (ORR: Up to 65%)
- Surgical excision: For readily accessible conjunctival or lacrimal sites
- IFRT (24–36 Gy): For disease in retrobulbar locations. 4Gy, followed by regular follow up may be tried to prevent complications such as cataract and xerophthalmia
- Advanced stage disease is treated same as advanced stage Gastric MALToma
Pulmonary/ bronchial MALT Lymphoma
Etiology:
- H. pylori
- Achromobactor xylosoxidans
- HIV
- HCV
- Sjögren syndrome/systemic lupus erythematosus
- Smoking
- Common variable immunodeficiency syndrome
Clinical features:
- Cough
- Dyspnea
- Chest pain
Additional evaluation:
- Bronchoscopy and bronchoalveolar lavage
- Esophagogastroduodenoscopy
Treatment of localised disease:
- Localised disease: Surgical excision. RT, if there is residual lymphoma after excision
- Advanced disease: Same as advanced stage Gastric MALToma.
MALToma of Salivary glands
Etiology:
- Sjogren syndrome
- IgG4 related disease
Additional evaluations:
- ENT examination
- US or CT or MRI of the head and neck
- Esophagogastroduodenoscopy
- Anti-SSA and anti-SSB antibodies
Treatment:
- Localised disease: Surgical excision or Involved field RT (RT is less preferred due to higher risk of worsening xerostomia and long term dental complications)
- Advanced disease: Same as advanced stage Gastric MALToma.
Colonic MALToma
Clinical features:
- GI bleeding
- Intussusception
- Bowel obstruction
- Mass visible on CT abdomen/ colonoscopy
Additional evaluations:
- Colonoscopy with tattooing (to facilitate localization of initial lesion)
- Esophagogastroduodenoscopy
Treatment:
- Localised disease: Polypectomy, surgical resection, radiotherapy
- Advanced disease: Same as advanced stage Gastric MALToma.
MALT lymphoma of Breast
Additional evaluations:
- Mammography and US, MRI
Treatment:
- Localised disease: Surgical excision or Involved field RT
- Advanced disease: Same as advanced stage Gastric MALToma.
MALToma of Thyroid
Etiology:
- Hashimoto’s thyroiditis
- IgG4 related disease
Additional evaluations:
- Ultrasound, CT scan of the neck
- Thyroid function tests
Treatment:
- Surgical resection with or without chemo-immunotherapy
EMZL/MALT lymphoma involving CNS
(Dura is commonly involved)
Etiology:
- IgG4-related disease
Clinical features:
- Seizures
- Headache
- Cranial nerve palsy
Treatment:
- ISRT or ISRT plus whole brain radiotherapy (WBRT)- 24–30 Gy
- Systemic high-dose methotrexate and non-HD-MTX regimens (with Rituximab): For rare patients presenting with secondary CNS MZL/ patients with parenchymal disease/ extra-CNS manifestations
Immunoproliferative small intestinal disease (IPSID)/ Small intestinal MALToma/ Mediterranean Lymphoma/ Digestive Alfa chain disease
Etiology:
- Campylobacter jejuni
- Helicobacter pylori
- Vibrio cholera
- Campylobacter jejuni
- Intestinal parasites
Epidemiology:
- Common in areas with poverty and poor sanitation
- Common at 20-30 years of age
- Common in men
Clinical features:
- Chronic watery diarrhea
- Weight loss
- Malabsorption
- Abdominal pain
- Finger clubbing,
- Vomiting
- Fever
Additional evaluations:
- S. Immunoglobulin levels: IgA is elevated (>3820 mg/L)
- Endoscopy: Duodenum is commonly involved, atrophic nodular mucosa, thickened mucosal folds and edema
- Biopsy: Lymphoplasmocytic infiltration of the lamina propria and villi blunting
- USG/ CT: Enlargement of mesenteric lymph nodes, thickening of the small intestinal wall, dilations and strictures of small bowel loops
- C. jejuni assessment by PCR, IHC, or ISH
- Stool parasite exam, stool culture test
- Helicobacter pylori breath test
Stages (based on histopathology):
- Stage A: Lymphoplamacytic infiltration of the lamina propria with inconstant and variable villi atrophy
- Stage B: Atypical lymphoplasmacytic infiltration of the lamina propria and atypical immunoblast-like cells spreading to the submucosa with subtotal or total villi atrophy
- Stage C: Proliferation of atypical lymphoid cells in all layers of the intestinal wall (generally large masses are present)
Treatment
- Antibiotics: Tetracycline/ Doxycycline alone or in combination with ampicillin or metronidazole for 6 months
- If no response/ systemic disease/ large cell transformation (stage B and C) use R-CHOP/ R-CVP along with antibiotics if not used earlier
- If bulky mass, consider surgery/ RT prior to starting chemotherapy
- Supplementation of essential vitamins, minerals and nutrients by parenteral nutrition
Hepatic MALT Lymphoma
Etiology:
- Hepatitis C virus
- Hepatitis B virus
- Other viral hepatitis
- H. Pylori
- Autoimmune hepatitis/primary biliary cirrhosis/Sjögren syndrome,
- Ascariasis
Primary cutaneous marginal zone lymphoma
Epidemiology:
- Accounts for 1/3rd of primary cutaneous B cell lymphomas
Etiology:
- Tattoo pigments
- Vaccines
- Tick-borne bacteria- Borrelia burgdorferi infection
- IgG4-related disease
Pathogenesis:
- Associated with FAS mutation
Clinical features:
- Presents as multifocal or less frequently solitary red or violaceous plaques or nodules
Histopathology:
- Dense dermal infiltrate composed of small lymphocytes, plasma cells.
- Follicles with reactive germinal centers may be seen.
- IHC:
- Positive: B cell markers, BCL2
- Negative: CD5, CD10, BCL6 and cyclin D1
Criteria for diagnosis:
- Essential:
- Presence of CD5-negative, CD10-negative small B cells.
- Demonstration of monotypic plasma cells, monotypic B cells, and/or clonal immunoglobulin gene rearrangement.
- No evidence of extracutaneous disease at the time of diagnosis.
- Exclusion of other cutaneous lymphomas.
- Desirable:
- Lesions on trunk or arms
- Reactive lymphoid follicles in lesion
Prognosis:
- Favourable. 5 year survival: >98%
- First-line antibiotic regimen: Ceftriaxone 2 g/day for 14 days
Treatment:
- PCR- Negative for B. Burgdorferi or Positive cases that do not respond to antibiotic, with localised disease: Involved lesion RT (24 Gy) or surgical excision
- Generalised lesions (Skin only)
- Skin directed therapies (Steroids, imiquimod, nitrogen mustard, bexarotene)
- Intralesional steroids
- Rituximab
- Advanced disease:
- Asymptomatic: Wait and watch
- Symptomatic: Chemotherapy- Rituximab single agent or combination chemotherapy
Nodal Marginal Zone lymphoma
Introduction:
- It resembles lymph nodes involved by marginal zone lymphomas of extra nodal or splenic types, but not associated with any extranodal or splenic disease.
- Careful history and physical examination are necessary once diagnosis is made, to rule out coexisting extra-nodal MALT lymphoma.
Epidemiology:
- Very rare
- Often occurs as spread from extranodal MALT lymphoma
- 1-2% of all lymphomas
- 10% of all MZLs
- Median age- 60 years
Etiology:
- HCV is positive in 20% cases
- Clonal B-cell lymphocytosis (CD5-, CD10-) is considered a precursor lesion
Clinical Features:
- Usually asymptomatic
- Localized or generalized lymphadenopathy
Investigations:
- Lymph node biopsy
- Marginal zone and interfollicular areas of lymph nodes are infiltrated by marginal zone B-cells, monocytoid B cells or small B-lymphocytes
- Scattered centroblast and immunoblast like cells are present.
- Diffuse/vaguely nodular pattern is seen
- Residual germinal centers are preserved, but are disrupted
- Immunohistochemistry
- Positive- CD20, CD19, CD79a, PAX5, IgM; BCL2 ; coexpression of CD43, MNDA, and IRTA1
- Negative- germinal center markers, LEF1, CD10, CD5, Cyclin D1, BCL-6
- Molecular studies
- Clonal rearrangements of immunoglobulin genes- VH3 and VH4 families are predominantly mutated
- MYD88 gene mutations- Absent (Helps in differentiating from LPL)
- Cytogenetics- Trisomies- 3, 18 and 7 , gains of 2p and 6p and loss of 1p and 6q
- t(11;18)- Absent
- Immunofixation electrophoresis: 10% have IgM monoclonal gammopathy
Criteria for diagnosis:
Essential:
- Proliferation predominantly of small, mature B cells with scant to moderate amount of pale cytoplasm, with or without plasmacytic differentiation
- Architectural distortion in a nodular/follicular, parafollicular, interfollicular, or diffuse growth pattern.
- Absence of markers supporting follicular lymphoma, mantle cell lymphoma or other specific small B-cell lymphomas
Desirable:
- Presence of markers such as MNDA or IRTA1
- Residual follicles with follicular colonization
- Detection of monotypic light chain expression in B cells and/or plasma cells.
- Detection of clonal immunoglobulin gene rearrangements
Prognosis:
- 60-80% survive for more than 5 years
- Follicular lymphoma IPI may used for prognosticating
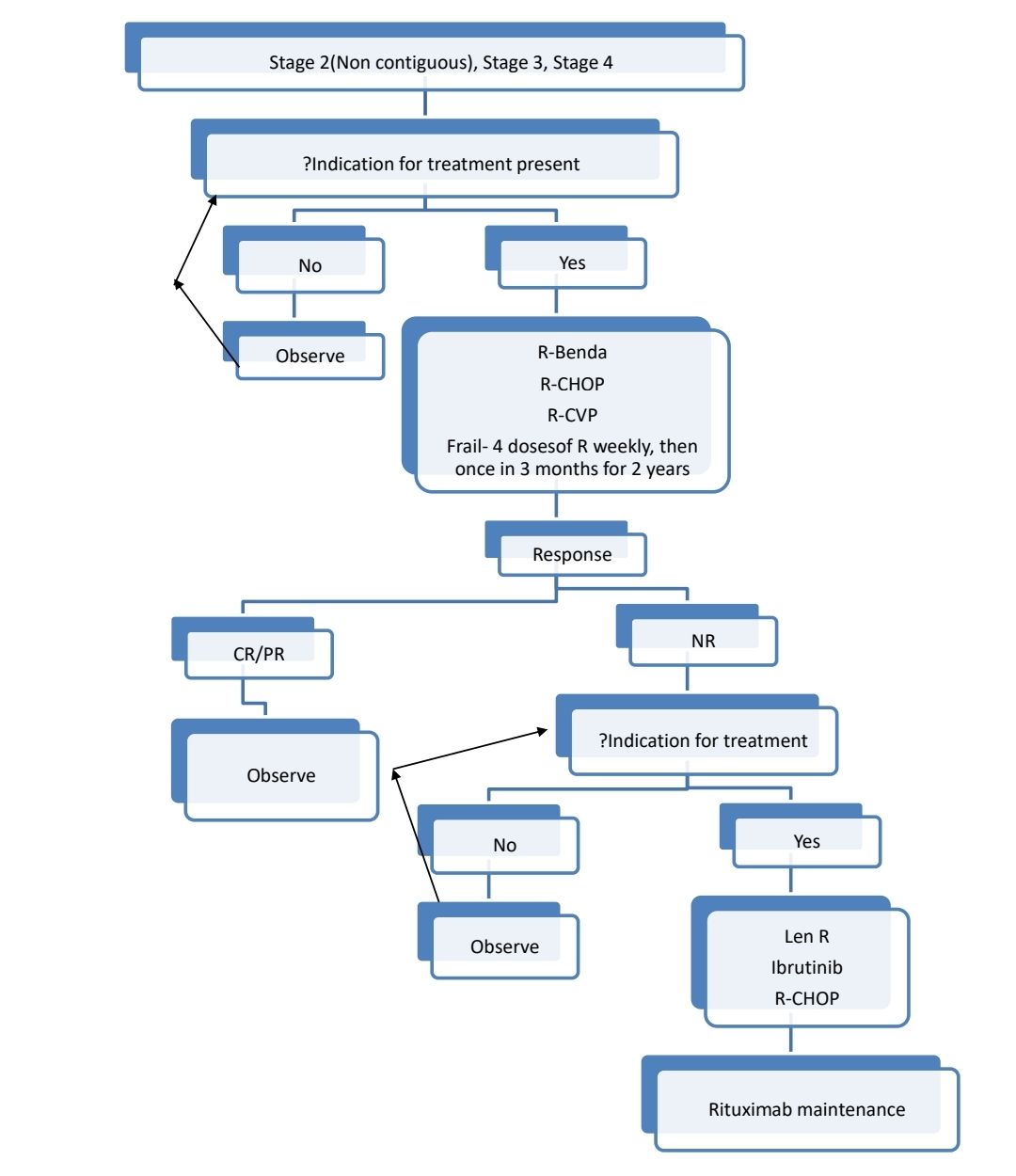
Indications for Treatment:
- Symptomatic patient
- Threatened end organ function
- Cytopenia secondary to lymphoma
- Bulky disease
- Steady/ rapid progression
Additional investigations prior to starting treatment:
- BM aspiration and biopsy in all cases
- Flow cytometry
Treatment Plan:
Limited disease- Stage I or Stage II (Contiguous)
- ISRT- Then assess response
- CR/PR- Follow up- If progression of disease treat as extensive disease
- NR- Treat as extensive disease
Advanced stage:
If HCV positive: HCV eradication leads to lymphoma regression in the majority of patients
Monitoring After Treatment/ Follow-up:
- History, examination and labs every 3-6 months for 5 years, then yearly once
- CT (CAP)- 6 monthly for initial 2 years, then once a year
Special Situations:
- Histological transformation
- Disproportionate increase in size of one particular node
- Increasing LDH
- Development of extranodal disease
- B Symptoms
- Treated as DLBCL/Double hit lymphoma. In both do HDT with ASCR
Pediatric nodal marginal zone lymphoma
- Mostly occurs in lymph nodes of head and neck region
- M:F= 20:1
- Asymptomatic
- Localized disease
- Criteria for diagnosis
- Essential:
- Partial effacement of LN architecture by interfollicular proliferation of marginal zone cells with monocytoid and centrocyte-like morphology
- Monoclonal IGH and/or IGK genes rearrangements;
- Immunophenotype compatible with marginal zone B-cells (BCL6-, CD43+/-).
- Desirable:
- Residual follicles with PTGC-like features
- Follicular colonization
- Monotypic light chain restriction
- Increased PD1+ cells in reactive germinal centers
- Increased PD1+ cells in reactive germinal centres
- Essential:
- Treatment: Localised complete excision is often sufficient. Rarely systemic therapy is needed.
- D/D- Atypical marginal zone hyperplasia with montypicIg expression
An Initiative of
Veenadhare Edutech Private Limited
1299, 2nd Floor, Shanta Nivas,
Beside Hotel Swan Inn, Off J.M.Road, Shivajinagar
Pune - 411005
Maharashtra – India

howitreat.in
CIN: U85190PN2022PTC210569
Email: admin@howitreat.in
Disclaimer: Information provided on this website is only for medical education purposes and not intended as medical advice. Although authors have made every effort to provide up-to-date information, the recommendations should not be considered standard of care. Responsibility for patient care resides with the doctors on the basis of their professional license, experience, and knowledge of the individual patient. For full prescribing information, including indications, contraindications, warnings, precautions, and adverse effects, please refer to the approved product label. Neither the authors nor publisher shall be liable or responsible for any loss or adverse effects allegedly arising from any information or suggestion on this website. This website is written for use of healthcare professionals only; hence person other than healthcare workers is advised to refrain from reading the content of this website.